Wednesday, June 17. 2009
No good deed goes unpunished.
Well, that is surely not always true, but with the economic downturn, the charity medical clinic at which I volunteer one day per week has seen a sharp upturn in lawsuits against us Docs and the clinic this year.
The medical defence lawyer we have now engaged (we have had no complaints or suits for 10 years until January 2009) tells us that we should now regard each patient as a potential enemy. (Our clinic's founding Christian philosophy is to regard every patient as a friend and neighbor.)
He tells us that our notes must be guided by the principle of CYA (your notes are legal documents, not medical reminders as we had thought) and that every decision a doc makes contains some basis for a suit in the hands of a hungry lawyer because all medical decisions are judgement calls and every situation is unique.
He also told us that recessions tend to see more suits against doctors because more folks are looking for cash, and much more so in charity settings. Plus the tort lawyers are hungry too - but they always are. He also advised us to refuse to treat any patients with substance abuse histories for our protection - other than alcohol.
He actually said "Do not be kind. They will screw you whenever they decide to." He has been around the block a few times.
I do not like this at all. A Psychiatrist/Psychoanalyst cannot do the job under such conditions. Furthermore, I can not and will not endure any relationship in my life without mutual trust. I am considering resigning (even though I was one of the founders of the place) and finding some other outlet for my charity. Maybe prison work, where you can safely begin with the assumption that everybody is a liar and cheater and working the system - and take it from there.
My position on the Board, plus my volunteer time (all unpaid) doubles my legal liability. I just want to do my best, tithe and double-tithe my time, and avoid hassles that do not fit into my life - and legal fees that I cannot comfortably afford.
And no, I would never work for ObamaCare. Never. I did not go into medicine to be a government employee. I went into medicine to work for my patients, doing my best, with no intention of looking out for lawyers.
Tuesday, June 9. 2009
It's tough for doctors because we are often held responsible for people who either do not want, or do not accept, our help and advice. But, as long as their name remains on our rolls and as long as we persist in trying to be constructive, the lawyers can get us.
I have been burned several times by keeping them on the rolls in the charity clinic, only to be sued by them eventually for not doing a better job "taking care of them." What? I am not a professional mother and I do not "take care of" anybody. I am a doctor, not a caretaker and, despite the modern lingo, not a "care-giver" either.
Like all doctors, I try to work with my patients - and do not take care of them, or I to try to bring them around to where I can work with them.
If I were more self-protective, I would not even try and would just say "I cannot help you. Good bye," but that is not my medical tradition. My medical tradition is that you are a friend to your patients, whoever they are.
Novalis presents such a case. More practical docs than I am would just throw them out of the office. However, after being punished and hassled legally several times by going the extra mile, my heart grows harder.
Indeed, good deeds often are punished and yes, it does lead to some bitterness especially when it is performed on a charity basis. I have never been sued or hassled by a private, self-paying patient.
Wednesday, May 27. 2009
Via Tiger at Althouse, Mary Roach (author of Stiff) with video on orgasms from fetus to death.
Friday, May 8. 2009
Another reminiscence from our shrink friend Nathan about his days in the Indian Health Service -
 A limp and a death among the Lakota Sioux marked my first day at Eagle Butte, devoid of eagles and buttes. Two daysÆ drive from Chicago, I am greeted from afar by John Running Horse, he dipping and rising like a Venetian gondolier, waving aloft what from afar seemed to be the plaster sculpture of a leg. Up close, it is. A limp and a death among the Lakota Sioux marked my first day at Eagle Butte, devoid of eagles and buttes. Two daysÆ drive from Chicago, I am greeted from afar by John Running Horse, he dipping and rising like a Venetian gondolier, waving aloft what from afar seemed to be the plaster sculpture of a leg. Up close, it is.
Before I could stop completely, John Running Horse lay one hand on the open window of my red Fiat 128, bowed in head and cast, asked, ōYou the new doc?ö I was. ōPut this thing on againö; hands me the cast, then points to his gondoliering leg. I park and head in.
The Indian Health Service had told me that there were two docs; arrive Sunday.
But, by Sunday, Dr. K. had been flown out with her atrial flutter to be cardioverted eighty miles up the road to Mobridge; Dr. L. was riding shotgun with a mother in active labor also to Mobridge. No docs in Eagle Butte.
I wrapped a new cast on John Running HorseÆs right leg and asked as I did so -- dipping plaster rolls in warm water, smoothing them first around, then smoothing downward along the fracture to make it seamless -- how his old cast got cut off. Itched, he said; cut it off himself, as he unsheathe his James Black/Musso pattern S-guard bowie knife. White plaster still dusted its curved Stainless steel back tip and brass quillion; hadnÆt even wiped it clean.
I told John Running Horse that his skin would itch again after a few days; dried skin flakes. I found a metal coat hanger, bent it straight and showed him how he could insert it within the cast to scratch itches. He found this marvelous; made a special leather sheath for it to hang from his belt. Later, he returned; brought a water color gift; painted himself on his horse; he wearing Sioux gear. In his right hand, born aloft like some victorious banner is not a leg cast, but his Winchester Model 1894 lever-repeating rifle -- the gun that won the West, the weapon of choice for the Rifleman of TV.
Continue reading "A Limp and a Death"
You used to just plain peter out at 68 or 79 or 93 but, after 1951, the law changed and some Doc had to make up a cause to put on the death certificate. A proximate cause, plus additional lines to fill in for contributing causes/underlying causes of death. (Imagine what that change did to disease stats!) More many more little-known facts about death.
Old time Docs knew that people died when they got old and rickety or had a bum ticker or some nasty growths. You plumb wear out eventually, and it is just a matter of which internal doohickey crapped out first. It was considered sort-of natural, and not a medical issue.
And, when folks died, they either said "They died" or "They ascended to their Maker" or "Went to their eternal reward." They did not say "They passed" (what a strange expression - passed what? New Agey-sounding, isn't it? Took a pass on more life, or what? Passed into the Spirit World?) or "passed away," as the relentlessly euphemistic funeral home people used to say. Like they aren't dead: they just sort of floated away past the 7-11 and the Pontiac dealership and the Pizza Hut to somewhere else.
Maybe to the lovely Mall in the Sky.
Tuesday, April 28. 2009
 The news mills are ginning up yet another medical crisis storm these days in an effort to pave the way for gummint medical care by the same good folks who run the DMV and the post office. They seem to imagine a problem with cost, access, and insurance. Maybe we are a nation of crybabies, because we have the best medical care in the world with which to pamper our so-called precious selves. The news mills are ginning up yet another medical crisis storm these days in an effort to pave the way for gummint medical care by the same good folks who run the DMV and the post office. They seem to imagine a problem with cost, access, and insurance. Maybe we are a nation of crybabies, because we have the best medical care in the world with which to pamper our so-called precious selves.
It's time we got beyond that self-love, and cared about the Greater Good. I have a few simple, rational, Utilitarian solutions.
Cost: Cost is driven by technology and modern pharmacology, cancer treatment, crocks (people obsessed with their health), gomers ("gomers go to ground"), and futile, guilt-driven end-of-life treatment for annoying old or sick relatives. The cost of American medical care can be dramatically reduced by forbidding all cancer treatment other than Oxycontin and at-home 10-gallon morphine pumps, all medical treatment for those over 57 (the children are our future!), all CT and MRI scans, all blood tests, and all medicines other than friendly, holistic, herbal organic ones. No more vaccinations - they cause Autism. No more antibiotics - everybody knows that they make people sick. Eliminate Dermatology (just stay out of the sun, people). Eliminate Opthalmology (bad eyesight is from masturbation - it's your own fault). Eliminate Psychiatry (mental illness is socio-political mind control). Eliminate Urology (do you want a #3 gauge tube stuck up your urethra?). Eliminate Surgery - it is physical assault on comatose victims. Eliminate Neurology - it's just nerves.
Access: Doctors are like waterfront trade unions: they limit their numbers to keep their payments high enough to join country clubs, to buy boats, and to take vacations. My idea: anybody who gets a C or better in Organic Chem is automatically admitted to a government medical school. Lots of good, caring people are weak in math and chem and bio and stuff, but that's who we need more of. My medical school flunk-out rate was 18%: what a waste of talent. Plus there are too many Jews and Asians in medicine anyway, and too few people of color or of gender identity diversity. So, with this increase in the numbers of docs, fees could go down to $5 per office visit and the docs who don't like it can open dry cleaning shops, cigar shops and wine shops like they do in Canada.
Insurance: Medical insurance is a dumb idea. Why expect your neighbor to pay your medical bills when they will be so low under my plan anyway? They will be cheaper than your garbage pick-up, your newspaper subscription, your cigarette costs, your car payment or your monthly payment for your big screen TV. (Did you ever notice how nobody complains about the cost of their TVs, computers, or Life Insurance?) Or just save your money if you want and die quietly without complaint, dude, and make space for the next generation. Too many people on the planet and, let's face it, life isn't all it's cracked up to be anyway. A vale of tears and toil, a tale told by an idiot, full of sound and fury, signifying nothing. What's the big deal about death? Didn't your parents teach you that life is a bitch?
Friday, April 24. 2009

Our shrink friend Nathan, who has completed Aliyah in Israel, sends this reminiscence of his days working for the Indian Health Service, doing general practice including surgery and obstetrics - and anything else that was needed. Old-timey medicine.
Before replacing the sloughed skin on Mrs. R's arm, I had to find out why her forearm was raw to the muscle. New here among the Sioux, I am surprised to learn that my colleagues (and one ancient Roman Catholic always fiddling with her rosary) hadn't checked this elderly, chunky widow's blood sugar: diabetic, sure enough, never diagnosed. So, first things first: stabilize her blood sugars, treat the diabetes, and give proper antibiotics (for anaerobes and aerobes -- they missed this too), then when you see the shiny, glimmer of healthy tissue margins, go for a skin flap transplant.
The pharmacist was my surgical assistant; he was the brightest of the bunch, from N'orlins, La before the Flood, he couldn't get into med school, he said, but he was smart, hard-working and pleased to assist. He also ordered special hickory chips from N'orlins, La. to barbecue and made his own roux. It was then that I learned I loathed ochra, that slimy matrix it exudes.
Then how to unskin a lady was not to be straightforward as it was at the University hospital where I studied. The surgical suite -- well-endowed -- had not been used for years; surgery was sent eighty-miles up-road to Mobridge to the White hospital; none done here, except deliveries (which too often evolved into C-sections who had to be sent, ambulance screaming, up to Mobridge. One trip, the eternally-soused obstetrician kept his fist in the mother's vagina to keep the baby from popping out.
To unskin a forearm means to find a donor site from the inner thigh. Anesthesia needed for this and there was no anestheiologist, no nurse-anesthetist, even in the 1970's. I do double duty. First, a lumbar block to numb the donor site; second, a brachial plexus block -- in the armpit -- to numb the recipient, the naked forearm. Lumbars I had done many of: babies with possible meningitis; Southside Chicago girls in active labor, with no prenatal care and needing an urgent C-section. But, brachial plexus block was a never-done for me; remembered the anatomy, the complex twistings and routings within that armpit, like some noodling of telephone wires beneath the city streets, but never stuck a needle there. The night before surgery, I bone-up on my Netter's anatomy and hit the spot square-on the next day in the O.R.
Before hitting the OR, I had done several days debriding of the sloughed wound: fresh it must be to transplant the sod of skin. In the OR, flipped on her side, I slid into the vertebral space between L4 and 5; a bit lordotic pull by the nurses and I had a clear tunnel in. Then, flapped on her back, Mrs R. was ready. The thigh well scrubbed, Betadined, aproned, an oval hole isolating the site. Instruments we had. The strange loopy-scalpel to slice just-thick-enough epidermis and a touch if dermis to both "take" to the new site, yet leaving some dermis to heal-over the thigh; something like a large cheese knife the instrument looked. Forearm next. Her arm flung up like some lop-sided angel wing, I probed left-handed with two gloved fingers, then slid the massively long needle --- like from the cartoons -- in between the stretch of skin. Wait. Wait. Numbness without paralysis in the arm. First, a touch on the skin (for sensitive fibers); then a pinch with a forceps (for the pain C-fibers) and success.
 Laying the layers onto the site is much like laying sod; carefully, side by side, the edges trimmed to the wound shape. The "root" growing will take on its own, a pressure bandage holding the skin sod in place. A fine lawn it will hopefully be; like sodding around a putting hole -- it should look good and cover the ground. And after five or six days of brief peeks, it looks darn good. Laying the layers onto the site is much like laying sod; carefully, side by side, the edges trimmed to the wound shape. The "root" growing will take on its own, a pressure bandage holding the skin sod in place. A fine lawn it will hopefully be; like sodding around a putting hole -- it should look good and cover the ground. And after five or six days of brief peeks, it looks darn good.
But, Mrs. R. wants a pass to leave early. There will be a Sundance ceremony with several initiants, including, I learn later, Russel Means, wanted by the FBI for shooting three men on Rosebed reservation, down south. I explain, I plead in fact, that she can't rotate the arm; she must stay in hospital a week or so until we know healing has happened. Mrs. R. has donated two buffalo for eats at the ceremony and insists, politely, quietly, firmly, that she is going. Wakantanka, the Sioux god whose voice one hears shushing through the Black Hills, will protect her. She invites me.
Being invited was one thing; getting in another. I and Debby were the only washichus, white men, attending. While this was a Lakota Sioux ceremony, it had become politicized; other tribes, mostly the more militant ones, as far away as the Navajo, had sent "guards": thick-armed toughs with long, greasy black hair and their image of mean on their faces. The fellow who greeted us -- we had the red Fiat 128 in South Dakota -- commanded us out. A face like a slab of steak with two eyes embedded, he frisked me; looking for drugs and guns, he said. His compatriots searched the tiny Fiat's baggage, checked under the carriage, beneath the seats, glove compartment. When he turned to frisk Debby, I told him firmly, no way: I would turn around and he could explain to Mrs. R. why I was not admitted. Her name was a key to the lock that was his harshness. We were passed through.
I did not expect to be the only Washichu; thought other docs would be invited; learned later that my do-gooder colleagues who come to save the Indians are not so welcome. Already, I had dispensed with making morning rounds with them, as I tired and was irritated at the "religion" they spouted at bedside; told them I needed to round earlier.
We formed a large circle. Formed is not quite right. A circle was somehow formed by the few hundred there, centered by the cottonwood from which leather strops hung. Each strop was anchored with a bone hook -- from what animal I don't recall, perhaps antelope. The six piercees entered; I'm told by Mrs. R. that they had purified themselves in the wild for several days with fasting and water. The hooks are pierced into the pectoral muscle, not the skin, to hold more firmly; one on each side. as the men leaned back against the leather thongs, faces skyward, Cubist, uptilting tits were formed: this manly ceremony giving rise to a touch of woman. A moaning or humming was emitted by them by these men; also those in the circle, as the men stomped sidewise about, a dance they called it, in a hypnotic slowness. A timeless quality it felt.
Near the end, several men appear with massive shallow wooden bowls, face us in the circle and pass around the dried buffalo donated by Mrs. R.
She is called to near the center. A peace pipe is to be given to her for her generosity. As some chiefly type raises the pipe, his arms extended, palms upward, I realize, a touch shocked, that she will now rotate her arms upward to receive the peace pipe with both hands. I feel a belly clutch: will she tear the stitches?
Mrs. R. looks back at me afterwards; tosses a smile of reassurance. Thanks to Wakantanka the skin is fine, she explains.
One weekend, we go to the Black Hills, find a cabin, rest outside beneath a sky filled with more stars than I have ever imagined. I feel a sense of annoyance as I hear the rush of what sounds like highway traffic just beyond the ridge. Ridge top I look: no highway; it is Wakantanka speaking through the black pine.
It was the only time He has ever spoken around me.
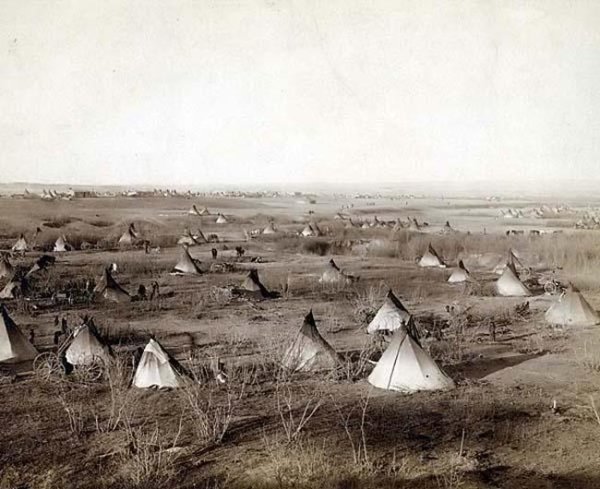
Top photo: Sioux war party, 1870s?
Middle photo: Sioux warrior
Lower photo: Sioux village
Friday, April 17. 2009
I opted out of Medicare years ago. I felt morally torn about doing so, but finally my bookkeeper refused to do any more of their paperwork. That settled it.
My compromise was to institute a generous sliding fee scale for Medicare-aged folks. (My general policy is to never decline a referred patient because of money.) From a young Doc, in the WSJ:
Here's something that has gotten lost in the drive to institute universal health insurance: Health insurance doesn't automatically lead to health care. And with more and more doctors dropping out of one insurance plan or another, especially government plans, there is no guarantee that you will be able to see a physician no matter what coverage you have.
Consider that the Medicare Payment Advisory Commission reported in 2008 that 28% of Medicare beneficiaries looking for a primary care physician had trouble finding one, up from 24% the year before. The reasons are clear: A 2008 survey by the Texas Medical Association, for example, found that only 38% of primary-care doctors in Texas took new Medicare patients. The statistics are similar in New York state, where I practice medicine.
More and more of my fellow doctors are turning away Medicare patients because of the diminished reimbursements and the growing delay in payments.
Monday, April 13. 2009
 Here's the real story about who is and isn't covered by medical insurance. Here's the real story about who is and isn't covered by medical insurance.
Not that the facts matter all that much in politics - and everybody wants a free Easter buffet.
Related: How the government plans to create its own medical insurance monopoly. (Just like public schools.) And once they have done that, they will drive through their rationing, rules, and controls. - and freedom in medical care will disappear. At that point, Doctor, your proud and noble profession will be transformed into involuntary servitude to the State rather than voluntary servitude to your patient and, at that point, patient, your treatment choices will disappear.
Then watch "doc-assisted" suicide for those over 60 become all the rage in government circles.
It's one more government power and money grab.
Thursday, April 9. 2009
 Yesterday morning's NJ post on "Quality Care" from the WSJ was enlightening, and just gives me one more reason to stay away from Medicare (besides the fact that they pay me peanuts, and that their paperwork requirements are over my head and take more time than my patients take). Yesterday morning's NJ post on "Quality Care" from the WSJ was enlightening, and just gives me one more reason to stay away from Medicare (besides the fact that they pay me peanuts, and that their paperwork requirements are over my head and take more time than my patients take).
I see how government "Quality Care" works: the academic medical experts take a vote, and that becomes "Quality Care." That's not medical care: that's government policy. Forget the individual patient and his or her unique situation, forget the Doc's experience and skills and insight, forget the Doc's judgement, forget the fact that academic Docs aren't always practical, forget that next week's new data will completely alter the information at hand. Just Follow The Rules and stay out of trouble.
I have seen plenty of cases go bad in the hands of young Docs who strictly follow the rules. It's not a good example of that, but when I was a resident one of "the rules" of the time included strict limits on the use of pain-killers, even for terminal cancer patients. Didn't want them to become addicts, you know. They forgot that pain relief remains one of a handful of the greatest blessings medicine has bestowed on humanity (along with anesthesia, antibiotics - and Lexapro).
One of the best things about seasoned physicians is that they are a cranky bunch who do not take orders, who think for themselves, who feel that rules are made to be broken, and who do not like to take crap from anybody - especially anybody in "authority". Your patient comes first, or you are nothing. There is a "House" inside every Doc. In most lines of work, you can't get away with that sort of attitude.
When government gets involved in things, they tend to screw them up. The article's example of high blood sugars in the ICU was a perfect example. Even I, who have not cared for ICU patients for more than a decade, know that tight sugar control for critical patients is insane and dangerous. Not only that, but it doesn't matter: if the patient survives and gets healthy, a few days of higher sugars with a good margin of error will not have hurt them one darn bit. But I am a Doc with a practical mind.
Expertise always has to be taken with a grain of salt, and government-emitted expertise with a tablespoon-full. I am not disparaging expertise, which I respect enormously. I just distrust the combination of expertise with power over others: anointed experts who want power instead of simply to educate give me the willies.
Non-"experts" often have loads of common sense. We take an ancient oath, too.
Ed. note: Somewhat related: Socialized medicine: A warning from across the pond
Wednesday, April 8. 2009
Mrs. BD had increasing pain in her right shoulder, then running down her biceps, for two weeks, finally keeping her awake at night. Gets an appointment with the #1 shoulder guy in the world at the Hospital for Special Surgery in three days (last Monday). He is a kind, caring fellow who takes time with her. She gets a shoulder MRI two days later. Gets the diagnosis of early frozen shoulder one day later. Begins physical therapy and anti-inflammatory meds one day later.
Feeling better already. Even Fidel Castro couldn't get that kind of care and help, nor could Obama get better. Do I want my neighbor to pay for this for me? No - but thanks so much for offering to pay her bill. I believe in taking care of my own.
The bad news for her: no tennis for at least 2 months. The bad news for me: I gotta do all the cleaning and scrubbing, right when it's time to begin enjoying yard and garden work.
Well, we have snow flurries today, thanks to global warming climate change, so I guess the gardens can wait a while.
Saturday, March 28. 2009
That's the latest cardiovascular recommendation for brisk aerobic exercise. (It used to be 20 minutes three times a week, but new data has changed that recommendation.)
I have not asked whether 30 minutes of vigorous sex five times/week counts, but we hope it does.
Tuesday, March 24. 2009
For some today, and for just about everybody in the past, medical insurance was something everybody bought, just like life insurance or disability insurance, to cover extraordinary expenses. It is called Major Medical, and it is still readily available.
Over the past 20-30 years, governments, businesses, and union contracts began expanding their coverage by reducing deductibles and covering more routine things. Medicare, of course, was the model for that. During the same time, costly medical technology and new drugs were developed in a near-miraculous way, mostly in the US.
With those changes, folks began wanting "insurance" to cover their routine maintenance medical expenses instead of the things that would financially overwhelm them. When that shift was combined with the CYA style of medicine which results in $5000 work-ups for dizzy spells (fed by the ambulance-chasers), everybody expected everything.
That isn't sustainable, and will never happen. Medical technology has grown to an amazing extent, but those machines are expensive.
I have no idea what the folks in power are trying to plan for us, but I know it will be an entitlement disaster, filled with unintended consequences, that people would not be happy with. It will end up with politically-determined rationing.
Our family bought Major Medical insurance many years ago. It cannot be cancelled. It's more important than a cool car. Why everybody does not do that when they are young and healthy is beyond me, because it would seem like the logical and prudent thing to do. Over the years, we have increased the deductible so that it is quite affordable, and we keep a money market savings account specifically for medical bills to the amount of the deductible. As I recall, we began with a $2000 annual deductible, and now we finally have a dirt-cheap $20,000 2-year deductible on the original policy. It does not cover any routine or preventive medical care, which is as I think it should be. Nobody owes me medical care, in my view, any more than anybody owes me auto insurance.
We have kept this policy whether or not I or my husband had some form of insurance through work, because you never know how long you will want to keep a position - or when you will be let go.
Off-topic: Around 30% of Medicare expenditures occur in the last year of life. In other words, on failing and terminal people. Interestingly and unsurprisingly, when docs hold end-of-life conversations with these patients (as we should), the costs go way down.
Wednesday, March 18. 2009
You can die of hypothermia when the temperature is well above freezing, and you will die of hypothermia after a while in 77 degree water. Many interesting facts at Freezing Persons Recollect (h/t, Cons Grapevine). All outdoorsmen should know this stuff. One example:
...many hypothermia victims die each year in the process of being rescued. In "rewarming shock," the constricted capillaries reopen almost all at once, causing a sudden drop in blood pressure. The slightest movement can send a victim's heart muscle into wild spasms of ventricular fibrillation. In 1980, 16 shipwrecked Danish fishermen were hauled to safety after an hour and a half in the frigid North Sea. They then walked across the deck of the rescue ship, stepped below for a hot drink, and dropped dead, all 16 of them.
Tuesday, March 10. 2009
George Bernard Shaw warned ōBeware of false knowledge; it is more dangerous than ignorance.ö The major overhaul of American health care pursued by President Obama and his supporters is based on many false premises and is excessive and likely to do more harm than good. Tuning up and improvements already always dynamically occurs. Instead, ObamaCare is aimed at dramatically changing one-sixth of the US economy in ways that are untested or tested and found wanting, primarily involving huge increases in government direction of health care.
The details of ObamaCare are largely being left to Congress, the same body that stuffs the federal budget with earmarks, waste, and other programs that are not requested. ObamaCare is premised on claims for drastic changes in health care and major increases in government programs being necessary. Those claims are largely specious.
Below the fold, the top ten specious premises for ObamaCare are discussed:
1. Comparing US Health Care To Other Developed Countries
2. US Health Care Spending Is More Than We Can Afford
3. Reform Overhaul Will Yield Major Savings
4. Increased Evidence-Based Medicine And Health Information Technology Will Significantly Improve Care and Reduce Costs
5. Present Administrative Costs And Insurer Profits Are Too High
6. US Consumer Dissatisfaction Requires Drastic Health Care Changes
7. Health Care Costs Are So High They Are A Major Cause Of Personal Bankruptcy
8. The Number Of Uninsured Is So Large That Drastic Health Care Changes Are Necessary
9. More Preventive Care Will Better Serve Consumers And Save Costs
10. Health Care Consumers Are Being Served By Drastic Health Care Changes
(More could be added, such as that government restraints on prescription drug prices will not impede incentives for innovations, but they are so transparently false that the list below dwells on other ObamaCare premises more misleading.)
Continue reading "Top Ten Reasons For ObamaCare Are Based On False Information"
Tuesday, February 10. 2009
Docs have been poo-pooing routine vitamin-taking for many years. We tend to think of it as a rip-off (although I do take a daily Vit D). Studies continue to indicate their uselessness in adulthood, but the placebo effect cannot be underestimated.
We linked the Bloomberg piece this morning describing what the "stimulus" will do to ration care under Medicare. Also in the stimulus will be a federal monitoring of your medical history and treatment - this from our Canadian friend at Small Dead Ducklings:
The billÆs health rules will affect ōevery individual in the United Statesö (445, 454, 479). Your medical treatments will be tracked electronically by a federal system. Having electronic medical records at your fingertips, easily transferred to a hospital, is beneficial. It will help avoid duplicate tests and errors.
But the bill goes further. One new bureaucracy, the National Coordinator of Health Information Technology, will monitor treatments to make sure your doctor is doing what the federal government deems appropriate and cost effective. The goal is to reduce costs and ōguideö your doctorÆs decisions (442, 446). These provisions in the stimulus bill are virtually identical to what Daschle prescribed in his 2008 book, ōCritical: What We Can Do About the Health-Care Crisis.ö According to Daschle, doctors have to give up autonomy and ōlearn to operate less like solo practitioners.ö
[...]
Hospitals and doctors that are not ōmeaningful usersö of the new system will face penalties.
If Obama screws up the American health care system, where the Hell are Canadians supposed to go?
If they want docs to give up their autonomy, they had better find a new, lesser breed of docs in this country. And I'd rather fight with an insurance company about my medical choices than fight with a federal bureaucrat. If the insurance company doesn't want to pay, I can at least pay for it myself.
Tuesday, January 6. 2009
General hospitals are increasingly relying on "hospitalists" to care for inpatients, freeing up office practitioner's time for their (steadily less lucrative) outpatient practices.
I have yet to be a hospital inpatient except for childbirth, but I think that, if and when I am, I'd like to see the face of my own Doc daily.
This is a new model for medical practice. More time-efficient? Probably. Less comforting? Probably. Overall, better or not? I cannot say.
Internists, and what few GPs still exist, are having a tough go of it these days: Medicare, which is the bulk of their work, compensates them now at a rate lower than a plumber or electrician in Boston.
Friday, December 5. 2008
Your doctor may be so concerned about protecting you from alcoholism that he or sheĀmight not tell you that current research indicates that 1-2 drinks per day appears to reduce the risk of heart and arterial diseaseĀby 18-30%. More is not better, however. Details at Medscape.
Monday, November 17. 2008
 We have posted on statins in the past. We have posted on statins in the past.
Here's further evidence that statins are helpful, regardless of your triglyceride levels.ĀMaybe all guys should take them (per your Doc's advice, of course.)
Wednesday, October 8. 2008
A piece on the subject in the NYT notes: The myth is that like magic, preventive medicine will simultaneously reduce costs and improve health.
Read the whole thing. Sadly, except at the margins, there is little we can to to prevent disease. The wishful thoughtĀthat we can control fate and the gods never quits, though.
Tuesday, October 7. 2008
From guest author Bruce Kesler:  ĀHealth care could be the next Fannie Mae type disaster.Ā Similar forces are at work, and despite the lessons that should be drawn instead may be accelerated by the current financial meltdown.Ā These forces are exaggeration of need and rights among the poor, greed by many of the rest of us, and many politicians seeking votes or contributions. ĀHealth care could be the next Fannie Mae type disaster.Ā Similar forces are at work, and despite the lessons that should be drawn instead may be accelerated by the current financial meltdown.Ā These forces are exaggeration of need and rights among the poor, greed by many of the rest of us, and many politicians seeking votes or contributions.
Ā The forces in the credit crisis were the appeal to provide opportunities for home ownership to the poor and the consequent inflation of housing values that provided paper gains to the middle class and wealthy.Ā Underlying these forces was a pyramid scheme profiting the political and financial elites that was dependent on trust in repayment of subprime loans by many without the means or stake in doing so. Ā Thus, ultimately the taxpayer and more careful consumers and investors are required to pay off, also making other worthy goals unaffordable.ĀĀĀĀ
Continue reading "The Fannie-ization of Health Care"
Thursday, September 25. 2008
 What's up with Beauty Studies (ie Neuroaesthetics)Āthese days? What's up with Beauty Studies (ie Neuroaesthetics)Āthese days?
A quote from Beauty and the Brain (by the proprietor of Neurophilosophy)Āin Seed (h/t, Dr. X): ...recent work by several researchers at University College London?Ś?including the establishment of the first major grant-driven research program for the neurobiological investigation of aesthetics, or neuroaesthetics?Ś?has made the first steps toward a unified biocultural theory of art. An object's beauty may not be universal, but the neural basis for appreciating beauty probably is. The researchers' initial discoveries and the increasing formalization of the field promise to open the way for the first time to an understanding of beauty based on something other than speculation.
Can things of the soul and spirit be understood in terms of neurotransmitters and neural wiring? Count me a skeptic. Different levels of organization have different rules and patterns which do not transfer one to the other. For example, you could know everything about atoms but never predict a living cell, and you could understand everything about a cortical network without predicting Moby Dick. (And, for me, on a good day I see beauty everywhere but on a bad day I see it nowhere.) Still, they may as well give it a try. I get skeptical when they call it a bio-cultural model, however. It makes itĀtoo clear that they seek to detour around the psychology part.
Monday, September 22. 2008
 How are your teeth? How are your teeth?
Teeth are a sensitive subject. When you lose one as an adult, you feel a bit emasculated. Lose a handful, and you can develop a clinical depression. And root canals are a torture which even the CIA would never inflict on Osama. My first one was without Novocaine at age 14. The elderly dentist didn't "believe in" Novocaine. I have had plenty since then. Plus it costs big bucks to keep good teeth after 45, unless you are one of the lucky ones with genetically strong enamel. My teeth are mediocre-to-poor. I have one implant so far, many crowns, and a number of failing crowns. My wisdom teeth were pulled years ago. I have some extractions andĀtwo moreĀimplants on the way,Āplus a bridge. Most of my teeth have fillings and miscellaneous repairs. My dentist blames it on cigars and bad tooth genes, and says I need a serious big-time periodontistry before he can do anyĀmore repairs and reconstruction. I also lost a few front ones playing hockey in prep school. The brother of my then-girl friend stuck the end of his stick in my face, entirely by accident no doubt. Whenever I am sent to a new person, eg a periodontist or an implantologist or an oral surgeon, before I open my mouth I always say "Promise youĀwon't say 'Oh my God what a mess.'" This stuff gets expensive. But even worse is that it is a depressing reminder of ones' aging and deterioration, a memento mori. Entropy alwaysĀwins. We pay and struggle, but we always lose the battle.
Thursday, September 18. 2008
People talk about the Canadian system (horrible for Docs and patients) and the NHS (which 56% of Brits want eliminated). Few discuss the way the French do it, but it's worth thinking about. Part 1 of Health Care Reform discusses the historyĀFrench system, noting "They emphasize private, fee-for-service practice even more than we do." If you are interested in the topic, Synthstuff links all 4 parts of this essay, written by a Doc who likes the system.
|

