Thursday, August 21. 2014
 We have commented on the subject of the human diet and health before, but it's time for another comment, because the NYT Science Times has written on it. We have commented on the subject of the human diet and health before, but it's time for another comment, because the NYT Science Times has written on it.
"Healthy food" has been an on-and-off American obsession, comparable to the obsession with flavor in France.
Since Rev. Sylvester Graham, a minister, vegetarian, and food-obsessive invented the Graham Cracker in the 1820s to provide "digestive fiber," Americans have been food faddists and vulnerable to food quackery.
More famously, Dr. John Kellogg of Battle Creek, Michigan, an 1870s charlatan with a diet fad, fooled Americans into thinking that cereal was breakfast food. It is not. In Yankee-land, breakfast is eggs, bacon, sausage, toast, potatoes, fruit and apple pie.
Eat what you want, and be happy. All humans are prone to "magical thinking" - aka "wishful thinking." We'd like to imagine that we have some control over things like health, and that things we put in our mouths will make a difference. There is essentially no evidence for that idea, assuming absence of a disease, or a problem like high cholesterol, or pregnant, etc.
Even being fat doesn't seem to make any significant difference to health. (Being obese is a bad plan, though.) I advise patients to eat plenty of salmon, trout and char for their magical properties, and whatever else they want; to exercise and work out if they want to be strong and fit but not because they will live forever; to lose weight if they want to look better and feel less tired; to eat all the salt and steak they want; and to avoid magical health diets. Vegetarian? Fine. Leaves more lamb and steak for me. Just don't imagine that it's about health. What's a healthy diet? Any average mix of stuff, but most of all - enjoy it, and don't fuss about it too much.
(Image from the excellent medical blog Kevin, MD. That steak could be a bit more rare, if you ask me.)
Saturday, August 16. 2014
An annual re-post -
 Why is the CDC based in Atlanta? Because Georgia was the center of malaria in the US, and elimination of malaria from the US was the CDC's first job. It's hard to imagine, but through the 1940's malaria was endemic in the southern US, and prior to that in the northeast too. Every doc in New England used to treat malaria routinely. Why is the CDC based in Atlanta? Because Georgia was the center of malaria in the US, and elimination of malaria from the US was the CDC's first job. It's hard to imagine, but through the 1940's malaria was endemic in the southern US, and prior to that in the northeast too. Every doc in New England used to treat malaria routinely.
DDT was a major factor in the elimination of malaria in the US, but it remains a common disease in the Third World, in the southern hemisphere. And, sadly, DDT harms lots of other things, too, besides mosquitoes but probably isn't as evil as Rachel Carson claimed.
The long history of malaria would make a fascinating book. I'll just share a few facts: the germ which causes malaise, fever, and anemia is a plasmodium, a wierd one-celled bug. There are 4 varieties. The vector (meaning the thing that distributes the bug) is of course an anopheles mosquito, which squirts the germ into the human bloodstream with its anticoagulating saliva. The plasmodium reproduces in your red cells, then goes loose in your blood, where it is presumably sucked up by an innocent mosquito who  spreads it further. Humans are the host of this bug (meaning their reproductive home). Like any parasite, the goal is to keep the host alive, while reproducing itself. If you kill your host, you sort of defeat your purpose (like over-taxing productive people), so malaria is more likely to cause chronic illness than death, except in the otherwise vulnerable. Fascinatingly, the sickle-cell trait of Africa confers resistance to malaria. Nature is amazing, which makes being an MD an astonishing privilege. spreads it further. Humans are the host of this bug (meaning their reproductive home). Like any parasite, the goal is to keep the host alive, while reproducing itself. If you kill your host, you sort of defeat your purpose (like over-taxing productive people), so malaria is more likely to cause chronic illness than death, except in the otherwise vulnerable. Fascinatingly, the sickle-cell trait of Africa confers resistance to malaria. Nature is amazing, which makes being an MD an astonishing privilege.
Prevention is simpler than treatment. Treatments include derivatives of sweet wormwood, as discovered in China in 300, and derivatives of cinchona bark (quinine), as discovered by the Spanish in the 1600s. The quinine treatment/preventative of course gave rise to the finest drink of the British Empire - the Gin and Tonic, which exemplifies the idea of making a virtue of necessity. A Brit will drink nothing without either gin or wine in it. Add a lime and the Limey can prevent scurvy too, as was attributed to Captain Cook. Thus truly a superior medicine for both body and soul.
Does the brand of gin matter? For martinis, yes. For gin and tonics, not to me anyway.
Saturday, August 23. 2008
Diagnostic errors remain the  leading reason - or excuse -Āfor medical malpractice lawsuits by the swarms of hungry sharks which parasitize American's fine physicians - the best physiciansĀin the world. Kevin, MD. leading reason - or excuse -Āfor medical malpractice lawsuits by the swarms of hungry sharks which parasitize American's fine physicians - the best physiciansĀin the world. Kevin, MD. All the more reason for docs to be irrational - or rationally irrational - in spending your money (either yours directly, or the insurance company's money - which was your money). If you have a headache, I am going to order an MRI of your headĀwhich will cost you between $700-1100 in my area. I know darn well that you don't have a tumor, but I could be wrong 0.3% of the time. So I'll order the MRI, because you will want me to, andĀmy law suit defensiveness will want me to. Still, I will know that it is poor medicine. Indeed, I know that your particular pattern of headache, and your examĀshows it to beĀa Common Migraine, and not a tumor, not an aneurysm, not a stroke or subdural, etc. And I know that all sorts of guidelines have been constructed, such as these.ĀWell, you can toss the guidelines for all I care. The Barrister'sĀrecent series on error (Part 1 - Fun with the Null Hypothesis,ĀĀ
Part 2 - False Positives and False Negatives, Ā
Part 3 - Risk of Inaction and Opportunity Cost)Ā applies beautifully to modern medicine. There is almost no endĀto the amount of your money we can spend to try to reduce our False Negative ratesĀ- our Type 2 errors. And they will occur, regardless.Ā It is very unpleasant to be sued. It damages a doctor's enjoyment of his art, it absorbs huge amounts of time and energy, and it damages his relationships with all ofĀhis patients. And, finally, it has nothing to do with his competence and everything to do with the greed and litigiousness of his patient.Ā I pay 42,000/year for malpractice insurance as a GP, and I have never been sued. I know guys who pay 160,000. You are paying those bills.
Saturday, July 26. 2008
A re-post from 2005: NormĀhas posted some interesting dataĀfromĀa recent study on theĀdifferences in libido between men and women. The results sound like that medical research spoof about the 20-year, 70 million dollar government study which proved the surprising fact that diet and exercise areĀimportantĀfor weight loss. This newĀstudyĀoffered the startling conclusion that menĀhave higher sexual needs than women. More specifically, the study says that men need sex every five days, and women every ten. My opinion:ĀThis studyĀonly applies to Brits.
Tuesday, October 17. 2006
Everybody shouldĀget some CPR training, with regular refreshers. You never know when someone is going to go down at the supermarket, in church, at the movies, inĀa parking lot,Āor at a baseball game. Be the person who knows what to do. In the tension of the moment, it's hard to think straight unless you are in an ER with support and help. And people collapse all the time, usually for minor and relatively benign reasons.ĀBut sometimes it's an arrhythmia, or a heart attack-related arrhythmia, and, if so, it's your chance to try to save a life as long as you aren't too far from definitive help. In the wilderness, forget it. They're a goner if they quit breathing. CPR is a temporary thing. Online CPR certification here.Ā(with sound). It's best to practiceĀit with a dummy, though. I have only had to perform this once in a non-medical setting. A rainy, cold, wetĀparking lot. She survived, but with mild brain damage from hypoxia (the cause of her collapse and subsequent respiratory failureĀwas a ventricular arrhythmia of unknown cause). And I cracked a rib or two, but that hardly matters when someone is "trying to die," as docs call it.
Wednesday, August 23. 2006
I had a friend who went through a hell of a time with a pulmonary embolism (a very commonĀlife-threatening andĀcommonly life-endingĀevent in all ages)Āfour days after a flight from Rome to New York. I would have thought that the stats were higher, but it appears that the occurrence of deep vein thrombosis (clot formation, in this case usually in the legs, which, when they get loose, are carried to the lungs) is only doubled during travel of four hours or more - whether car, plane, bus, etc. The solution might be a baby aspirin, but best is to keep those legs moving a bit instead of sitting immobile for long trips. Get up, walk around, stop the car and walk in a circle, whatever. Or just twitch your legsĀrestlessly the entire trip, as if you had ADHD. That will help prevent this terrible problem.
Tuesday, August 22. 2006
 I do not post often enough, so I am grateful that Bird Dog keeps me on the Soros-sponsored payroll. I do not post often enough, so I am grateful that Bird Dog keeps me on the Soros-sponsored payroll.
Our worthy and self-sacrificing editor emailed this piece to me from Stumbling and Mumbling, a pleasantly cantankerous economics-oriented Brit blog. Apparently the Brit NHS has a euphemistically-named "National Institute for Health and Clinical Excellence," (does that sound like something out of Brave New World?)whose job is to decide what treatments the government will pay for with your tax dollars. They try to apply cost-benefit analysis to your problem. Of course, such a process necessarilyĀpoliticizes medical treatment by making every treatment, and every disease, a political football, with the loudest voices and the squeakiest wheels and theĀmost patheticĀstoriesĀwinning out. And also turns every person into an expense item on a spread sheet, thus making it cost effective for everyone to die promptly without burdening their neighbors, at the precise moment when they cease to generate tax revenue. Citizens become, in essence, farm animals on a government plantation. The potentially-fatal flaw in democracy is that people can vote themselves "free" stuff, because there is no end to that childish wish. But with each "freebie," there is a loss of autonomy, of self-reliance, of adulthood, and of freedom. American patients are accustomed to have their problems insulated from government cost-benefit committees. They are accustomed to freedom, which can cost a bit more. And if theyĀrequire low-cost or free care, they can go to any clinic they want, almost everywhere in the US. I work in one, for nothing, in Providence, one day a week, and have done so for 20 yearsĀ- but you have to prove that you are poor. You may not take advantage of our good intentions. And if you sue us, you can, should, and will,Āgo to hell. Well, that was a digression from the point at Stumbling that I wished to highlight. He noted that no other government "programs" are subjected to cost-benefit analysis, except for medical treatments. Now, you just have to wonder, why might that be? I have faith that, in general, Americans will never sell their freedoms for a bowl of lentils.
Wednesday, August 2. 2006
 To a Fat Lady Seen From the Train To a Fat Lady Seen From the Train
O why do you walk through the fields in gloves,
ĀĀĀĀ Missing so much and so much?
O fat white woman whom nobody loves,
Why do you walk through the fields in gloves,
When the grass is soft as the breast of doves
ĀĀĀ And shivering sweet to the touch?
O why do you walk through the fields in gloves,
ĀĀĀ Missing so much and so much?
Frances Cornford wrote that -Āthe charmingĀform isĀcalled a triolet. Our editor asked me to comment on Dr. Helen's piece on fat people. As a doctor, I tend to be a "Do as I say, not as I do" sort of guy. I smoke cigars and I am pleasantly, or some might say prosperously, or some might say, grandfatherly, well-fed. When patients of mine are seriously overweight, I tell them straight out. The word fat does not bother me. I have a model in the waiting room of five pounds of adipose tissue designed to get a reaction. It is disgusting. As someone who did my share of general surgery earlier in my career, I can tell you that fishing through gallons of yellow adiposity, getting your gloves so greasy you cannot hold the scalpel, is no damn fun. If you are fat, and saw whatĀyou look like under the skin, you would be horrified. Another complication recently published is that obesity makes it more difficult to make a diagnosis. It's called "study or exam limited by body habitus." However, I also understand that the flesh is weak, and that staying in youthful shape after 45 is no mean feat. It takes work and discipline, and the evidence that it leads to longevity or health is minimal. However, being in good shape adds a lot to quality of life. On the other hand, being obsessed with health is for the crazies. Plus there is the vanity factor:Āfew guys will look at a fat girl, and no gals will look at a fat guy - unless he is rich or powerful. But, at some point, unless we are narcissists, we accept reality and don't care all that much. Final word: If you are too fat, I will say that. And, if you care, I will tell you how to deal with it. But your life choices are not my problem, beyond that: your doctor is not your Momma, nor is he/she responsible for your health. Your health is in your hands, and God's, and nature's. My only responsibility is to give you advice as your friend, and to try to help you when you get sick.
Thursday, July 6. 2006
Is it moral to sell your kidney? Your placenta for stem cells (or does it belong to your kid?) What are the ethics - if any - and morals of commerce of the human body? Which is an indirect way of asking what the morals and ethics of capitalism are. We know what many libertarians would say, but what would each of us say? Eric Cohen at New Atlantis has a fine wide-rangingĀessay on the subject, covering Calvin, Voltaire, Weber, Adam Smith, Irving Kristol, etc etc.: Biotechnology and the Spirit of Capitalism. Couple of quotes: In 1991, with the last vestiges of communism crumbling and the Cold War ending, Irving Kristol warned that the greatest threats to a capitalist future were spiritual and cultural. ōIn a sense,ö he said, ōit is all Adam SmithÆs fault. That amiable, decent genius simply could not imagine a world where traditional moral certainties could be effectively challenged and repudiated. Bourgeois society is his legacy, for good and ill. For good, in that it has produced, through the market economy, a world prosperous beyond all previous imaginingsŚincluding socialist imaginings. For ill, in that this world, with every passing decade, has become ever more spiritually impoverished.ö In the end, SmithÆs error was his lack of ōeschatological realism.ö Man is not simply an average being who seeks to improve in material ways. He is also an imperfect being who yearns for perfection, a mortal being who yearns for immortality, and an ambitious being who sometimes believes that he can make others more perfect or less mortal through his own mastery of nature. And so Adam SmithÆs world of practical commerceŚa great successŚis still haunted by the Protestant desire for other-worldly grace and by VoltaireÆs desire for ōterrestrial paradise.ö We demand that material progress offer salvationŚwhich is exactly what socialism once promised and what biotechnology may promise in the future. Or we demand that material progress be abandoned in the name of salvationŚsoberly, by those who seek to preserve sacred retreats in a profane world, or radically, by extremists who seek to dismantle modern life altogether.
Read the whole thing. It's an education.
Wednesday, June 14. 2006
 As a guy who has been in practice for many years, I have no doubt that doctors' decisions are the reason American medical attention is as expensive as it is. As a guy who has been in practice for many years, I have no doubt that doctors' decisions are the reason American medical attention is as expensive as it is.
However, what Kling in his excellent and important piece at TCS omits is the extent to which such decisions are driven by patients and their families. Most patients, offered the option that "this might help," opt for it. And the docs go along with it, even if the statistical gains are marginal to none. In other words, they replace their measured judgement with the "consumer's" choices. "Doc, do everything you can." I see it every day, and haveĀdone thisĀcountless times myself. And why not, if someone else is paying the bill? Do we love outselves too much? Or do we want to believe in magic? (Also, bear in mind that the physicianĀordering your test or procedure makes no money from that.) As a consequence of "consumerization" and litigation, the band of "elective" procedures and tests shrinks ("elective" used toĀimply that Major Medical insurance would not pay for it), while the band of the routine expands, including the marginal, the useless, the "heroic," the hopeless, the experimental, and the optional. Many extremely expensive cancer treatments would be on that latterĀlist, plus allergy "treatments," plus even routine annualĀphysicals which I believe are a waste of time and moneyĀ- my list would be quiteĀlong, and I could easily annoy every medical specialty. In the good old days of medical authority, before people came up to you and said "I read on the internet that there's a doctor in Arizona who says...", physicians were capable of carrying the burden of making good decisions for their patients. And when folks were ready to go, we let them go: we would never treat pneumonia in the ICU in Alzheimer's patients. That is not rationing - that is sane decision-making. And we all pay the bill. Thus American medical care is more expensive, but minimally more effective, than other places: we spend our extra money on the margins, and on terminal patients, where outcome is not meaningfully affected. A classic example comes to mind: Mickey Mantle, with metastatic lung cancer and dying, gets a liver transplant for his cirrhosis. I doubt a physician recommended that, but they probably did say it was an option, and he said "sure." It probably gained him a couple of weeks of torture and misery, in the hospital. Kling considers all of the possible causes for medical costs, and concludes: That leaves (D), with its radical suggestion that America's culture of medical practice is at fault. I arrived at this conclusion as an economist, looking at the data that contradicts the alternative hypotheses and also at a variety of studies, cited in my book, that show little relationship between health care outcomes and the supply of medical services. Since writing my book, I have come across the work of Nortin Hadler, an MD who, coming from a very different direction, arrived at the same conclusion that I did about America's medical culture. In 2004, Hadler published The Last Well Person: How to Stay Well Despite the Health-care System Hadler takes on many popular forms of health care in America, from alternative medicine to colonoscopy screening to anti-cholesterol drugs to heart bypass surgery. In his iconoclastic view, all of these therapies have benefits that are too small in terms of either statistical significance or common sense to warrant widespread use (he qualifies this by saying that certain narrow target populations do in fact benefit from these approaches). Hadler steps on some very sensitive political toes. Americans want to hear that our doctors "save" men with prostate cancer. Hadler sees it is a common, slow-acting ailment that can be left untreated (there is a less-common variant that is more dangerous). We want to believe that talk-show hosts who scold people to get mammograms, watch their cholesterol, and submit to the indignities of colonoscopies are doing the public a service. Hadler argues that we should take a more stoic attitude toward the risks that we face.
Please read the whole thing.
Saturday, April 8. 2006
Anytime the government gets involved in do-gooder projects, they screw it up. Their motive is generally some combination of "caring" and vote-buying, and the effect is usuallyĀa reduction of freedom and choice, a diminution of personal responsibility, and numbers of people working the system. I am not convinced that there is any huge national demand for more government involvement in medical care. We already have Medicaid for the poor, and Medicare for both the wealthy and the non-wealthy older folks. More and more doctors are opting out of Medicare, though. I no longer accept it, mainly because the coding is impossible to understand, and if I make a mistake, it is a felony. I would rather offer charity when needed, as docs have done forever. But I no longer do any costly procedures. However, medical practice has changed, and the costs of procedures is large. Every responsible person should have Major Medical coverage these days unless you are so wealthy that paying $20,000 for a bypass, or $16,000 for a hospital stay after being hit by a truck, or $100,000 for a dubiously-effective long drawn out treatment for metastatic cancer, is easy for you to pay out of the checking account. In addition to the costs of running a hospital these days, and the cost of procedures, there is no doubt that concerns about law suits have increased the cost of medical care. Prudent and practical medical judgement becomes replacedĀby fear-driven decisions, resulting in enormously expensive tests in search of the 1-in-10,000 possibility. Thus, between the costs of malpractice insurance and the cost of low-probability tests, trial lawyers, insurance companies, and hospitals are the beneficiaries of medical insurance. They all get paid. Who are the people who really "need" Major Medical insurance, but lack it? Not the poor - they are covered. Not the over-65 - they are covered by their under-65 neighbors via Medicare taxes. Not the prosperous - they buy it, or are insured through work.ĀIt's the under-65Ānon-poor (and their families)Āwho have eitherĀnot arranged their lives in such a way as to buy orĀto obtain coverage through work -Āand illegals. Plus those with chronic problems who cannot buy insurance and are unemployed. That is who we are talking about when we talk about the "uninsured." In Mass.,Āmost of the uninsured turn out to be young single men who don't want to spend the money on it - their foolish choiceĀshould not be our problem. A healthy married couple, both working at Walmart, with a family income of $56,000, can certainly afford to buy medical coverage, although it might mean driving an older car. In my opinion, any medical insurance law ought to recognize that those are the targets for it. Also, any medical insurance law should be Major Medical - with a choice of deductibles anywhere between $500-10,000. And no coverage for quackery and elective things such as chiropractic, yogurt enemas, homeopathy, gym memberships, abortions, routine check-ups, herbal wraps and massage "therapy." While everyone wants a free lunch, there is none. Somebody pays the bill - either you, or your next-door neighbor pays it for you. As I always say, if you want to have a body, and kids, then figure out how to take care of them. It's part of being a grown-up. Do what you have to do, and make good choices. Life is hard. Nobody promised us a rose garden.ĀĀUtopian dreams of government "solutions"Āusually end up turning into nightmares, while emptying our pockets, nurturing an un-AmericanĀsub-culture of weakness, dependency and entitlement,Āand reducing our freedom.Ā If you cannot take care of kids, or would rather buy a new car, do not have kids. It's your choice. They can be expensive, but do not dump their expenses on your next-door neighbor. That is lame unless, due to grieveous misfortune, you need charity. Americans love charity, but they hate to be ripped off by people with options. Kesler has a follow-up piece on the Mass. laws, looking at its shortcomings. And a conservative Mass. reader offers a fine rant in our Comments about the unwelcome burdens of government's efforts to do things for him. Recent posts on the subject: Scroll down. Other pieces we have done on the subject here and here. Image: MRI of the head. Cost: $400-800. There happens to be a brain inside that one.
Wednesday, April 5. 2006
A MassachusettsĀreader offers this: What are you guys smoking over there? Here I am in Massachusetts, without health insurance, and with a family of four, and all that has happened is on top of having to pay full freight for my family's doctor bills, I get fined $1000.00 for the privelege.
I don't want your stinking welfare greenstamp department of motor vehicle government cheese copay paperwork foodstamp prepaid doctor tax charity ward let a millionflowers bloom supervision of my family's medical situation, thank you very much.
Catastrophic medical insurance is currently illegal in Massachusetts. All they had to do is allow me to purchase what I could get if I lived 50 miles west, which is REAL LIVE INSURANCE, that is, they would pay if something unexpected, substantial, and expensive happened. And it would cost me a couple hundred bucks a month. But no, I have to pay full freight for every lamebrain thing that every knucklehead who has a job with benefits wants tax free, like gym memberships and aromatherapy and acupuncture and reiki massage and "mental health," ie, I'm a miserable failure as a human being and I want to talk to another miserable failure that went to community college for psychology about it, at great expense. Oh, yes, let's not forget all middle age men that need free blue pills because what a mean spirited thing it would be middle age men didn't wander the earth with extra free hardons.
And so "insurance" becomes paying in advance for others to get what they don't need or deserve, to the point where "Insurance" costs 1200 a month and if something catastrophic did happen, would bankrupt me anyway, because instead of paying $50 for an office visit for an imaginary ailment, but having a real catastrophe paid for, the powers that be would prefer paying $5 dollars copay for an office visit to their yogurt enema wellness healer, but have to chip in 20% for cancer therapy, which would bankrupt anybody that has to worry about the cost of health insurance in the first place.
I am totally sympathetic to what you are saying. I wrongly assumed it was catastrophic health insurance, which used to be called "Major Medical", which is the only kind of medicalĀinsurance that makes sense to me. Perhaps we are too gentle with the People's Commonwealth. I am not in favor of insurance for yogurt enemas or yoghurt massages either. What are we smoking? Upmann Magnums.Ā(We call it mid-dayĀ"relaxation-inhalation" therapy, paid for by ourĀinsurance, of course.)
Massachusetts has a new medical insurance law. I don't understand it all, but Bruce Kesler likes it, and he studies these things. The key is that you are required to be insured. Like with car ownership - if you own a body, you have to insure that darn thing yourself so you don't dump your maintenance costs directly onto everyone else. And taking care of one's healthĀand one'sĀfamily's healthĀisĀa greater source of pride than taking care ofĀthe car - or should be. Interestingly, it turned out that most of the uninsured in Massachusetts were young single men - they figure they are invincible, and they would rather buy beer and cars and F150s and deer rifles and Ezra Pound poetry and new outboard engines.Ā That is natural - irresponsible, but entirely natural. I don't think it will have much effect on the private practice of medicine, so that is a good thing. Hospitals will like it: they will get paid. And people should like it, because it keeps politics out of medical care...hopefully. Read Kesler's piece here. This could be ground-breaking. PS: Welcome, HH readers. Check out our blog - we are sure you will want to bookmark us! Our April Fool's Day satires were pretty good. PSS:ĀDissent from a Massachusetts reader - scroll up.
Wednesday, March 29. 2006
Do you have AdultĀADD? Take this quick test: 1. Do you sometimes get up to get something out of the refrigerator while watching TV? 2. When reading a technical text or doing homework, do you sometimes wish you were watching The Sopranos, or going to bed, or going out with friends? 3. When you have a huge pile of bills and paperwork, do you think "Aw, shit"? 4. Have you ever clicked "OK" or "I Agree" or "Next" on a website without reading all ofĀthe information? 5. When you are supposed to be focusing on something tedious, do you ever think about sex or other kinds of fun? 6. Have you ever opened a box from the bottom instead of the top? 7. Have you ever used a digital cameraĀwithout memorizing the manual first? 8. Have you ever had trouble finding your keys? 9. Have you ever stared out the window, thinking "I'd rather be fishing?" 10. When you are online, do you move from site to site without spending at leastĀ15 minutes perusing Maggie's Farm in detail? If your answer is "Yes" to one or moreĀof these questions, you definitelyĀhave ADD. See a doctor immediately before it gets worse.
Friday, March 24. 2006
Since around three pandemics occur each century, it is inevitable that a next one will appear. But will it be of the H5 bird type? Research over the past year suggests not. It is comforting to know that this flu is a greater danger to birds than to people, unless you spend a lot of time with infected birds. So as the mediaĀdramatically report the movement of H5 flu in birds, this seems to be more of ornithological interest than human-medical.
Tuesday, March 14. 2006
Roe v. Wade provided a "right" to kill an unborn baby for any reason. The morality and politics of that decision remain alive and unresolved. The decision failed to abort - or should I say "kill" -Āthe issue. In fact, it raised more moral and political issues. One effect has been to take a lot of the fun out of, and to add a lot of financial risk to,Āthe practice of Obstetrics. The concept of "wrongful birth" captures it. From an importantĀpiece in the NYT: At present, courts in about half the states recognize wrongful birth as a subset of medical negligence or allow lawsuits under the more general malpractice umbrella if a doctor's poor care leads to the delivery of a child the parents claim they would have chosen to terminate in utero had they known in time of its impaired health. In some of these states, like New York, where the Brancas' case was tried, emotional damages Ś compensation for the distress incurred by having an impaired child Ś cannot be recovered. No matter the legal context, terminating a wanted pregnancy is no one's first choice, but for the time being at least, when faced with a fetus that will become a severely handicapped child, all the choices are bad. At this moment, we are fairly adept at finding chromosomal flaws and horribly inept at fixing them. There is no chemical or surgical remedy if you find out your child-to-be has cystic fibrosis, fragile X, Down syndrome, Tay-Sachs, anencephaly Ś the list goes on and on. As Leon Kass, former chairman of the President's Council on Bioethics, has noted, in prenatal cases, often the only way to cure the illness is to prevent the patient. The first significant wrongful-birth lawsuit involving a disabled child, Gleitman v. Cosgrove, reached the New Jersey Supreme Court in 1966. One plaintiff was the child's mother, who had contracted rubella early in her pregnancy in 1959. Worried, she consulted her doctor and was assured that her unborn baby would be fine, despite the common understanding that rubella early in pregnancy can lead to birth defects. The baby in question was born with "substantial defects. . .in sight, hearing and speech." Interestingly, the court recognized the physicians' failure as well as the parents' anguish and attendant financial burdens although it still decided in favor of the defendants, in part, it seems, because it did not want to enter the ethical thicket inherent in finding for the parents. "A court cannot say what defects should prevent an embryo from being allowed life.. . ." the opinion reads. "Examples of famous persons who have had great achievement despite physical defects come readily to mind, and many of us can think of examples close to home.. . .The sanctity of the single human life is the decisive factor in this suit in tort. Eugenic considerations are not controlling. We are not talking here about the breeding of prize cattle." By 1978, however, when the next significant wrongful-birth case was decided by a higher court, the 1973 Roe v. Wade decision had established a woman's right to choose Ś that is, to terminate a pregnancy. The new case, Becker v. Schwartz, involved a geriatric mother (a medical term for a pregnant woman over 35) who was not advised by her doctor that her advanced age put her unborn child at greater risk for birth defects. Her child was born with Down syndrome, and shortly thereafter the mother sued. This time, the New York State Court of Appeals found in favor of the family, declaring it had the right to seek financial damages for the added cost of raising a child with a disability. The court, however, refused to allow the claim of emotional damages. It did recognize the family's suffering, but reasoned it "may experience a love [for their child] that even an abnormality cannot fully dampen."
Thursday, March 9. 2006
 The H5N1 Bird Influenza is spreading during the bird migration, as predicted. None in the Western Hemisphere, yet.ĀThus far, this will be a problem for those handling birds, and bird farmers. Be careful with your pheasants this fall, Mr. Free Market. The H5N1 Bird Influenza is spreading during the bird migration, as predicted. None in the Western Hemisphere, yet.ĀThus far, this will be a problem for those handling birds, and bird farmers. Be careful with your pheasants this fall, Mr. Free Market.
There is no evidence of a mutation which could endanger human populations on a large scale. Kill your parakeet and parrot and make a nice little soup out of them - and hope for the best. There may have been some hysteria about the Bird Flu - but it remains a risk that hangs over all of us. (Image: bird-fancier planning Cockatoo Stew for dinner.)
 The problem with vaccines is lawsuits. Companies are afraid to make vaccines. And in the current environment when quacks and trial lawyersĀblame vaccines for everything from autism to ADD to ingrown toenails, the manufacturers don't have a prayer with an Alabama jury. The problem with vaccines is lawsuits. Companies are afraid to make vaccines. And in the current environment when quacks and trial lawyersĀblame vaccines for everything from autism to ADD to ingrown toenails, the manufacturers don't have a prayer with an Alabama jury.
Why should they bankrupt their companies by trying to help people? I have been around long enough to remember polio. Folks, getting vaccinated for disease is your choice. But only a true ignorant fool would not have their kids vaccinated in these times. The problems began with the famousĀCutter Case. The all-knowing Dalrymple covers the medico-legal story in a book reviewĀin City Journal. Update: Just stumbled into this piece on the subject on the excellent Overlawyered blog.
Friday, February 10. 2006
Western Civilization malesĀare widely afflicted with this debilitating disorder. The cause is unknown, but some theorize that it is caused by the "Hen Flu," which shrivels up the testosterone-producing cells in the testes, along with the tubules which carry the hormone to the blood. Active research is going on in Australia, because this presumably viral ailment has not arrived there as of yet, making the study of uninfected males easier. However, it is unfortunately endemic in European, American, and Canadian males, and is transmitted, we believe but cannot confirm, by an unfirm handshake and a tendency to smile too much. It appears to be male-specific. Many of the symptoms are behavioral rather than physical, suggesting that the virus attacks areas of the brain as well as the testes. Typical behavioral symptoms include reflexive submission to aggression, eagerness to please, lack of pride, quick abandonment of familial heritage and ideals, a fear of firearms, absence of normal male drooling over attractive females, absence of normal male patriotism, Āand a deterioration of the instinct to defend family and compatriots. All can be summed up by the Omega Male Syndrome. Typical physical symptoms include occasional cold-like symptoms, the occasional cough, and fatigue, especially late at night and after drinking sessions. The only two reliable tests for this disorder, until the viral antibodies are further identified, are the Drool Test and the Adrenaline Response Test. In the former, test subjects respond to scantily-clad strippers, while measuring devices record saliva production, hardness of privates, and tendency to touch and sexually harrass. In the latter, test subjects are handed a military M16 while target images are passed by the target range. The number of holes in the Islamo-Fascist Jihadist imageĀseem to be a reliable measure of the progress of the disease. The only known cure is to read Maggie's Farm daily. Multi-million dollar studies by the CDCĀare ongoing to determine the mechanism of this therapeutic effect. The CDC is hopeful that these studies will further our understanding of brain-body interactions.
Wednesday, January 18. 2006
Very disappointed to see some of my favorite Justices on the wrong side of this one. This is not to make any medical point, even though itĀis medicalĀpractice across the USA to non-assist pain-ridden dying patients to "comfortably" slip away on morphine. My point is political: this is a state issue. Like abortion - if a state wants it, it's up to them, despite all of the complex moral considerations. Power to the people! Not to the Feds, who have no monopoly on wisdom or life experience. May I refer our readers to Amendments lX and X ? Having said that, though, I'd hate to see us become a country where the ill andĀinfirm are expected to go away to save us money andĀtrouble and inconvenience - which is what abortion is about, as I see it. That would be aĀBrave New World.
Friday, January 6. 2006
"Health Care" Never, ever, use the term ōhealth careö in my presence.
There is no such thing, and the words - and whatever concept, if any, which lies behind them - is anathema to me.
A word to the wise: medicine is an art, not a science. Yes, it is built on science, but it goes far beyond science which is why it is more of a priesthood than engineering. Not to disparage engineering, which I respect enormously. But the entire concept of the kind of Internist/GP medicine which I and many others practiceĀis built on an idea of an intimate relationship and committment to an individual person and their life.
Medical treatment does exist, and so does ōhaving a doctorö to keep an eye on your life and physical and emotional well-being and to take a professional/personal interest in your life, and especially in any "lack of health". Nothing called ōhealth careö does any of those things.
Doctors care about you; "health care" is an industrial/economic/bureaucratic concept in which you are little more than a potential expense item, but preferably a profit center ¢ whether the "system" - to borrow a socialist concept - Āis a government monopoly or an HMO or insurance company or whatever.Ā The industrial/economic concept does not ōcare,ö nor does it ōprovideö ōhealth.öĀ Only God and nature can provide health, and only a physician with whom you have a personal relationship, and with whom you have a personal contract, will ōcareö about you, because that is what they were made for.
In the modern-day ōhealth careö environment, I am beginning to see that people have deeper and longerĀrelationships with their electricians and plumbers (and I am not referreing to Lonely Housewives) than they do with ōhealth care providers,ö and it burns my ass, because that is not what being a physician is all about. It used to be that the specialists were the ones without the long-term relationships with patients: you were referred to them for a particular purpose, which they addressed, and then they came back to you. Nowadays, with ōhealth care,ö there is no ōyouö to come back to. When I see what is happening to Medicine today, it makes me want to cry.
Let me just tell you this: when I had my heart attack at 64 and my doc came into the ER and checked my EKG and said "Ed, it's an MI but you're gonna be OK and get back to work in a week or two", from a guy who had known me for 20 years, it meant more than you could imagine.
If the ōhealth care consumerö wants doctoring to be a cheap commodity offered by a randomĀDr.-of-the-dayĀōhealth-care providerö, well, itÆs their choice. Do not come to me for that. I believe I have much more to offer than that. But health ¢ that I do not have for sale. No-one can sell that. And ōcareö is never for sale, is it?
Tuesday, December 13. 2005
Whiners andĀAmbulance ChasersĀ The reason I cannot get any more flu shots this winter is because American drug companies no longer wish to make them. Why? Fear of law suits and side-effects. If a company is sued and hassled out of existence, they won't make anything for us,Āwill they? When the whiners, hypochondriacs and con-artists team up withĀthe trial lawyers for their mutual enrichment, watch out. The reason I can no longer prescribe an excellent drug, Vioxx? Law suits. Same with silicone breast implants for post-mastectomy people, now finally available again after driving Dow Corning bankrupt (because the whole legal case was a con job). My list goes on and on. Oh - and for a really big one - Tamiflu. Who's making it? Not one of the great US pharmaceutical innovators, no - Roche. Buy some, if you can - good luck. If law suits drive Merck out of business, there will be two big losers: the American patient and the shareholders - and a handful of extremely big winners: the lawyer-predators for whom it is no more than PR that they help "the consumer." Pure BS - they help themselves and themselves only. Like that bozo whathisname - the dopey smileyĀguy with the hairdo and dental workĀwho made many millions from cerebral palsy, as I recall, andĀran for VP with cut-and-run Kerry. You cannot preach to the trial lawyers - it's just a good slip-and-fallĀgame to them. But patients need to know that all medicines and medical procedures have risks and side effects. We may as well just tell you that anything could go wrong with you if you take an aspirin - because it's possible. You could bleed out your stomach, become hypotensive, and have a stroke, then fracture your skull on the bathroom sink as you fall, and break your arm when you land on the floor. It's happened. There is no benefit in life without a risk - however small. Life is not safe, and bad luckĀshouldĀnotĀrequire involuntaryĀcompensation from your neighbors. Voluntary help? Definitely.ĀDr. Miller has a good piece on the subject at TCS: One quote: RegulatorsÆ increasing sensitivity to safety concerns -- sometimes at the expense of the availability of essential drugs -- may have become contagious: Drug manufacturers, too, seem to have begun to ōerr on the side of safetyö to a degree that causes safe and effective drugs to be taken off the market voluntarily.
Consider Tysabri, only the sixth medication approved -- and the first in several years -- for the treatment of Multiple Sclerosis (MS), a debilitating autoimmune disease that affects the central nervous system. The stunning results of the drugÆs testing in clinical trials -- the frequency of clinical relapses was cut by more than half -- induced FDA to grant accelerated approval last fall. MS patients eagerly put their names on waiting lists to get the medicine.
But this ray of hope for MS sufferers was short-lived. By the time that several thousand patients were being treated with Tysabri, three confirmed cases of a rare neurological disorder caused by a virus were reported. (Because the drug suppresses certain aspects of the immune response, regulators, clinicians and the drugÆs developers had from the beginning been sensitive to the possibility of infections as a side effect.)
Immediately -- some would say prematurely -- the manufacturers of the medicine voluntarily halted production and distribution and withdrew Tysabri from the market. MS victims and many neurologists were bitterly disappointed.
Read the whole article.
Thursday, November 3. 2005
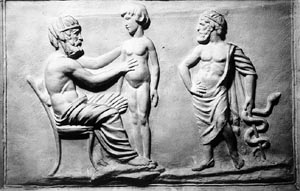 Asclepius, Asclepius, with his trademark one-snake staff,Āoverseeing a physician on a Greek frieze. (see piece below)
The Caduceus of HermesĀand the Staff of Asclepius These are two entirely different things which look similar. The caduceus,Āa traditional symbol of Western medicine, is in fact the staff of Hermes and has nothing to do with the 1200 BC Greek physician Asclepius, who was later deified, as the Greeks were wont to do with their impressive people. The caduceus story in brief: Tiresias, the blind seer and soothsayer, was said to have tried to separate two copulating snakes with his staff, which act transformed him into a woman until he was able to undo his act by repeating it, making him the first serial transgenderista. (Fair warning to snake-handlers.) Somehow, this staff, with the two snakes in love, was passed on to the god Hermes (Roman Mercury), the messenger god and the escort of the dead. (Hermes was a derivation from the Egyptian bird-headed god Thoth, to whom is attributed the authorship of The Book of the Dead.) The word caduceus is a derivation of the Greek karykeion, or "herald's staff." The association of the caduceus with medicine was an odd one, as in the 1600s Hermes was taken on as theĀsymbol of alchemy (hence "hermetic", referring to magic and the occult) and hence to medicine. The more appropriate symbol of medicine, and increasingly in use,Āis the staff of Asclepius, the god of healingĀ- one snake only and no wings of Hermes. The Asclepia were the Greek medical schools (Asclepion - singular) and healing centers. Was the original sign that Greek physicians hung at their doorways a worm on a stick, signifying their ability to de-worm people? It's not clear. But the asclepia were known for keeping non-venomous snakes around, for some reason. Pets? More detail on the subject here - a piece which I was surprised to find addressed exactly what I had intended to.
|