We are a commune of inquiring, skeptical, politically centrist, capitalist, anglophile, traditionalist New England Yankee humans, humanoids, and animals with many interests beyond and above politics. Each of us has had a high-school education (or GED), but all had ADD so didn't pay attention very well, especially the dogs. Each one of us does "try my best to be just like I am," and none of us enjoys working for others, including for Maggie, from whom we receive neither a nickel nor a dime. Freedom from nags, cranks, government, do-gooders, control-freaks and idiots is all that we ask for.
We're in Maine with iffy internet, lots of fish chowdah, clam chowdah, mussels steamed in white wine with garlic, wild blueberries, corn on the cob, and no hurricanes.
Where are our readers this week?
Can you say "no" to your kids? We do it, and have done it, every day. It's one simple syllable. Learning limits is a painful part of growing up but we all get past it in time. As we shrinks like to say, "Reality sucks." It is also beautiful, and so much of life is free, no charge.
The real achievement in life is not in saying No to one's kids, but in saying No to oneself. We call it "internalizing" the limits of reality and coming to peace with them. Who, at times, would not chose to be a kid again?
McCloskey's books were among my favorites as a kid, and favorites of my kids too. Make Way for Ducklings! Blueberries for Sal! It's real New England Yankee, Maggie's Farm stuff.
Swimming in Maine? It is not for the weak. You have to have the Right Stuff. Failure is not an option. Ya gotta join in.
With a little luck, both the brain and the mind can continue to mature throughout life - until decay sets in. A life trajectory is never set in stone. The brain will mature as it will, but the maturation of the mind and the emotions requires effort, discipline, and, most of all, rigorous self-criticism.
...nowadays there is a new science of happiness, and some of the psychologists and almost all the economists involved want you to think that happiness is just pleasure. Further, they propose to calculate your happiness, by asking you where you fall on a three-point scale, 1-2-3: “not too happy,” “pretty happy,” “very happy.” They then want to move to technical manipulations of the numbers, showing that you, too, can be “happy,” if you will but let the psychologists and the economists show you (and the government) how.
On a long view, understand, it is only recently that we have been guiltlessly obsessed with either pleasure or happiness. In secular traditions, such as the Greek or the Chinese, a pleasuring version of happiness is downplayed, at any rate in high theory, in favor of political or philosophical insight. The ancient Chinese sage Zhuangzi observed of some goldfish in a pond, “See how happy they are!” A companion replied, “How do you know they are happy?” Zhuangzi: “How do you know I don’t know?” In Christianity, for most of its history, the treasure, not pleasure, was to be stored up in heaven, not down here where thieves break in. After all, as a pre-eighteenth-century theologian would put it—or as a modern and mathematical economist would, too—an infinite afterlife was infinitely to be preferred to any finite pleasure attainable in earthly life.
And
Ominously... happiness studies have been diverted into an applied science. The happiness measurers very much want to direct us and are itching to engineer a happy society. They do not know what they are talking about, but are very willing to put “policies” about it into practice anyway. In a finely argued but erroneous book of philosophy, for example, Daniel Haybron a few years ago made a case partly on the basis of the new science of happiness against what he calls “liberal optimism,” or the belief since the eudaemonic movement and the bourgeois revaluations of the eighteenth century that “people tend to fare best—and pretty well at that—when empowered to shape their [own] lives.” He doubts it. But on what basis, since psychology is singularly ill-equipped to yield such doubt? As Haybron himself points out, tests on college kids do not range across enough experience. History is more to the point. Of course people make mistakes about their lives, and sometimes spend their lives badly. But as even Haybron acknowledges, the liberal experiment since 1700 has yielded gigantically better lives in every sense for a constantly increasing number of us. Haybron, and many of the elite critics of how other people spend their time on Earth, is an admitted pastoralist and disdains the sick hurry of modern life. Yet is he himself not living a happy life, which his ancestor around 1800—who in any case died in childhood and childbirth—did not?
It's a major essay. As I have said here many times, "happiness" cannot be defined in an applicable way beyond simple-minded gratification, but unhappiness is easy to recognize. It's everywhere.
"The narcissism of small differences" was Freud's 1917 term for his observation that people with minor differences between them can be more combative and hateful than those with major differences. It is a handy concept.
He viewed this as a narcissistic issue because the distress comes from looking in the mirror, as it were, and seeing a pimple.
What it is about is that we want all of "us" to think exactly like us - that is, perfectly, and the "others" be damned - who cares? Until the "others" give us big trouble.
Freud's psychoanalytic "movement" was repeatedly fractured by such things. Pioneers advanced into the human unconscious, and focused on different aspects, and fought and lost friendships over it. In the end, Freud was usually correct, because he had the courage to tell the often-unpleasant, unpopular, and uncivilized truths about deep human nature.
Of course, the narcissism of small differences often applies to politics. But my best joke on the subject concerns religion:
I was walking across a bridge one sunny day, and I saw a man standing on the edge, about to jump. I ran over and said: 'Stop. Don't do it.' 'Why shouldn't I?' he asked. 'Well, there's so much to live for!' 'Like what?' 'Are you religious?' He said: 'Yes.' I said. 'Me too. Are you Christian or Buddhist?' 'Christian.' 'Me too. Are you Catholic or Protestant?'' 'Protestant.' 'Me too. Are you Episcopalian or Baptist?' 'Baptist.' 'Wow. Me too. Are you Baptist Church of God or Baptist Church of the Lord?' 'Baptist Church of God.' 'Me too. Are you original Baptist Church of God, or are you reformed Baptist Church of God?' 'Reformed Baptist Church of God.' 'Me too. Are you Reformed Baptist Church of God, reformation of 1879, or Reformed Baptist Church of God, reformation of 1915?' He said: 'Reformed Baptist Church of God, reformation of 1915.' I said: "Die, heretic scum," and pushed him off the bridge.
In the LA Review of Books, Andrew Scull on All We Have to Fear: Psychiatry's Transformation of Natural Anxieties into Mental Disorders.
It's a good summary of what has been going on in my field these days. One quote:
This reliance on symptoms, and on the simplistic approach of counting symptoms to make a diagnosis, creates a bogus confidence in psychiatric science. Such categories have an element of the arbitrary about them. When Robert Spitzer and his associates created DSM III, they liked to call themselves DOPs (data-oriented persons). In fact, DSM’s categories were assembled through political horse-trading and internal votes and compromise. The document they produced paid little heed to the question of validity, or to whether the new system of categorizing mental disorders corresponded to real diseases out there.
It seems to me that stories confer value, or at least meaning, generally. Not just to objects. The brain is a creative machine, as Eric Kandel says. We indeed live in stories: stories about ourselves, our families, books, movies, songs, legends.
My work is all about stories. I rarely worry about objective truth during my workday unless I am concerned about being lied to. My concern is with psychic themes and subtexts.
In my non-work life, I care a lot about truth and rebel against self-serving "narratives" presented to me in advertising, by politicians, or anywhere else. As a shrink, I have a pretty good BS Detector.
In my field of study, work, and interest, the wonderful Roy Schafer made a major contribution to the field by highlighting the analytic attitude towards the patient's story. He noticed that the life story, and the day's story, changes as maturity and insight develop. Donald Spence's Narrative Truth And Historical Truth condenses many of these themes.
Politicians, activists, and the like have learned the power of narrative from the Psychoanalysts and the authors, and bent its power to the dark side. Propaganda no longer has simple big lies. Now it has whole stories which appeal to emotion for self-serving purposes, usually money, and/or power over others.
Propaganda, whether commercial or political, now appears as manufactured story-lines. "Truthiness," and all of that. Mark Twain: "A lie can travel halfway round the world while the truth is putting on its shoes."
The solipsistic fallacy is that there is no truth, just psychological truth. While that is often the Psychoanalytic approach to the soul and mind of a patient, when applied to the real world it becomes insane, and possibly dangerous.
Being a natural-born, many-generational New England Yankee, I have to confess that I have disdain for "relaxation." Engagement with life can be passive or energetic.
Don't blame me: it's my culture. We must respect different cultures, and Yankees value effort.
Over the years, I have come to realize (slow-learner that I am) that energy level is a major determinant of success in pursuing one's goals. IQ? Not overly important. Physical appearance? Important only at the margins although being tall does help. Education? A slight edge up, but only for your first job.
Here's how I assess peoples' level of life vigor:
1. Play computer games? Low vigor by definition
2. Watch over 1 hr. of TV/day? Low vigor
3. Read at least book per week? Good mental vigor
4. Read Maggie's Farm daily? Good mental vigor
5. Play sports instead of watching sports? High vigor
6. Make music instead of listening to music? High vigor
7. Exercise daily above and beyond walking (or hold down a physical job)? High vigor
8. Work under 60 hrs/week? Low vigor
9. Sleep after 6 am? Low vigor
10 Live on takeout instead of home-cooked? Low vigor
I need to work on this and produce a copyrighted "Vigor Score." I'll get rich off of it, and annoy millions in the process.
Thanks to Mr. Vanderleun for finding this, the only extant recording of Dr. Freud speaking. Despite the current zeitgeist, his legacy and his students have provided powerful tools to help suffering people and to understand human nature.
I started my professional activity as a neurologist trying to bring relief to my neurotic patients. Under the influence of an older friend and by my own efforts, I discovered some important new facts about the unconscious in psychic life, the role of instinctual urges, and so on. Out of these findings grew a new science, psychoanalysis, a part of psychology, and a new method of treatment of the neuroses. I had to pay heavily for this bit of good luck. People did not believe in my facts and thought my theories unsavory. Resistance was strong and unrelenting. In the end I succeeded in acquiring pupils and building up an International Psychoanalytic Association. But the struggle is not yet over. -- Sigmund Freud.
The very good Whittle video we posted this morning revealed that government in the US provides an average of $65,000 annually in funds, "benefits," and entitlements to poor families in the US. (Little or none of this is counted as income in calculating US poverty stats, as far as I know, nor, of course, does it take into account off-the-books cash income which seems pretty common these days.)
That's roughly the yield of a $2 million trust fund invested at a safe 1-3%, if my assumptions are correct. It's not a hard sale to convince people to vote for their own $2 million trust fund delivered by magic unicorns.
(The current fad for easy Disability and food stamps - anybody can get these things right now and I receive calls daily asking me whether I do Disability forms - is a whole new arena for free stuff, but a different topic. No, I do not do Disability forms on principle because I believe everybody is capable of dignity and self-respect. Speaking of cash, I have been offered good hard cash to fill them out for people in the last couple of years. On the phone "Doc, I'll pay you $1000 cash to complete my form for me.")
I have had plenty of experience with trust fund people, and am even fortunate enough to be the recipient of a very modest one myself, far less than $2 million in capital due to generational dilution. While some use their trust fund luck for productive purposes, many, it seems to me, lead relatively unproductive if not decadent, purposeless, and unstructured lives. People with meaningfully-sized trust funds, and families on the dole, have more in common with eachother than either has with the middle class.
As we often say here, real life is scary and challenging for almost everybody else. I am not convinced that that is a bad thing. It's the nature of real life and helps bring out the best in us. People spend money for lottery tickets just to enjoy the momentary fantasy of security and ease. Security and ease are infantile fantasies in this world which presents one problem after another.
Progressivism, in the Marxist and post-Marxist forms that have been swallowing the world for a century, is, in its methodology, nothing but the moral infantilization of mankind. It seeks the establishment of a population dominated by the childish fear of facing the world alone. Its pretty slogans are all variations on this theme. From "Workers of the world unite" to "It takes a village," the message is always the same: you can't face this "dog-eat-dog" world without the safety of the herd, which means without material security provided by political force. An all-powerful mother government must always be there to protect you from the ever-present monster, which is just life itself. And such security is not "charity"; it is your right. You are entitled to it, as any child is entitled to his parents' protection.
Today's ever-expanding "entitlement mentality" is literally shamelessness elevated to the status of a moral code. Progressivism has created an entire euphemistic vocabulary to justify the unabashed demand that others sacrifice their liberty to save me from my childish fear of facing life as an adult. "Positive rights," "social justice," "redistributive justice," "creative individuality," and so on, are all part of the leftist lexicon of cowardice.
Read it all. My view is that every American kid is born with a trust fund: their body, mind, soul, opportunities, and the remarkable free culture at hand. Amazing gifts which are rare on this planet. With all of that, nobody needs to lead a life which wastes his talents and capacities, or neglects his spiritual development.
I should add that I have no problem with trust funds per se (and have doubts about the whole idea of inheritance taxes too, which hit small family farms and businesses but never the very wealthy. America should welcome and ecourage family wealth-building, which reduces dependency). Similarly, I have no problem with the safety net for the very poor and/or dysfunctional. I do find it remarkable that American poverty benefits net out higher than the average American worker's income, which, like a good-sized trust fund, can be a perverse incentive for the weak in spirit. That's a shame, but people make their choices and not all Americans, unfortunately, have absorbed the American "Can Do" attitude.
Governments are marketing the "You Can't Do" attitude. It sells.
I mentioned The 48 Laws of Power a couple of weeks ago, labeling it "A Sociopath's Handbook." I now have my hands on a copy. It is, indeed, instructive in understanding what some of the people around us are doing. Here are some of the "48 Laws" that the book discusses:
- Never outshine the master - Never put too much trust in friends; use your enemies - Conceal your intentions - Always say less than necessary - So much depends on reputation - guard it with your life - Court attention at all cost - Get others to do the work - but always take the credit - Make other people come to you - use bait if necessary - Win through your actions, never through argument - Infection: Avoid the unhappy and unlucky - Keep people dependent on you - Use selective honesty and generosity to disarm your victim - When asking for help, appeal to their self-interest - Pose as a friend; work as a spy - Crush your enemy totally - Use absence to increase respect - Keep others in suspended terror; cultivate unpredictability - Isolation is dangerous: Do not build a fortress to protect yourself - Know who you're dealing with: do not offend the wrong person - Do not commit to anyone - Play a sucker to catch a sucker: Seem dumber than your mark - The surrender tactic: Transform weakness into power - Concentrate your forces - Play the perfect courtier - Re-create yourself - Keep your hands clean - Play on peoples' need to believe to create a cult-like following - Enter action with boldness - Plan all the way to the end - Make your accomplishments seem effortless - Get others to play with the cards you deal - Play to peoples' fantasies
1. Overheard from a wise old(er) RN in the ER this morning, "She's dying. Let her be."
2. Hospital bill for one of my patient's daughters for a 3-day ICU stay after an overdose: $124,000 (not including the bills from the numerous specialists who consulted on the case). That's the price of high-tech combined with tort fears. Tort-sensitivity prevents common sense in medicine, and results in rigid one-size-fits-all (expensive) protocols.
3. One-day ER bill for a stumbling drunk on the street brought in by the police after shouting to strangers that he was going to throw himself in front of a car: $3200. One wonders what happened to good old drunk-tanks at the police station. ER staffs prefer that drunks and addicts intoxicate themselves quietly without drawing attention to themselves.
4. An OR friend emailed me this pic of a nurse friend posing jauntily with surgical sponges. People have to have a little fun and humor in the OR. Fighting over what music to play is sometimes the most fun. Every OR has its CD player. Generally, the surgeon picks unless he or she is feeling especially generous towards the anesthesiologist or the nurses. Surgeons who want opera drive everybody else crazy.
I happen to believe, based on experience, that the right psychotherapeutic approach, tailored for the individual, can be enormously helpful.
Two of my favorite quotes:
Freud (often misquoted): "The goal of psychoanalysis is to convert neurotic suffering into everyday (ordinary) misery."
Erik Erikson: "Psychotherapy begins where common sense ends."
Readers know that I am a Psychiatrist (MD) Psychoanalyst whose practice is mainly in psychodynamic psychotherapy, less of a "medical model" practice.
Dr. Dworkin (an anesthesiologist and pundit) has a good summary of the the evolution of psychotherapy in America: Psychotherapy and the Pursuit of Happiness. A quote from his essay:
Psychotherapy has undergone a great transformation since America’s mental health crisis began. Gone are the days when therapists were dedicated to the doctrines of Freud and Jung, when the field was suffused with an air of priestly sanctity, heavy with the odors of tradition and authority. In the old days, psychotherapists constructed vast philosophical fabrics out of the writings of visionaries. They dallied with ideas that bordered on philosophy and religion; their emotional natures were totally absorbed in the partisan passions of their analytic cliques; their subtle intellects concerned themselves with the dialectical splitting of dogmatic hairs. The words they used — id, ego, and superego, among many others — seemed like a transcendent manifestation of divine power, an example of humanity being vouchsafed glimpses of eternal truth flowing down through an elaborate and immense cascade of books, with individual therapists stretching back, through their pedigree of technique, to some godhead. A whole universe of understanding was brought about by means of these words. In this universe the therapist was not as his clients, but, instead, a creature apart.
In the past few decades, a new breed of therapist has emerged — sympathetic, friendly, lighthearted, warm, and caring. His therapeutic style bears everywhere upon it the signs of human imperfection. It is the outcome of efficiency and practicality, of the exigencies of business executives and the ambitions of professionals, of the preferences of society and of the necessities of unhappy people. Gone is the transcendent manifestation, the abracadabra of therapy. Gone are the fervors of piety, the zeal of disciples, and the enthusiasm of intellectuals imagining themselves to have discovered a new theory of human nature.
Once a consecrated priesthood, therapists today walk along the smooth road of ordinary duty. They help people with their everyday problems. They speak in a casual manner and even crack jokes. They are friendly. They smile. They differ neither outwardly nor inwardly from the clients they serve, for whom therapy has become a useful organization, a convenient and respectable appendage to existence, a sometimes necessary form of artificial friendship.
I would cheerfully dispute the notion that physicians no longer constitute a priesthood of sorts, and I would dispute the notion that most people practicing psychotherapy, regardless of their training, are mostly busy with people with "everyday problems." (Some are, most aren't.)
As for "happiness," that's not something either physicians or "caring professionals" have the power to deliver. Relief of unnessary suffering and problematic behavior is difficult enough in itself.
In my view, psychotherapy is a deadly serious endeavor with the ambitious goal of rescuing lives and souls from their emotional problems and limitations, as much as possible. More like a mind-surgeon than a paid friend.
There are limits to the "medical model" of Psychiatry. Psychiatrists like me tend to focus on the "psycho-social" aspect, while others go full-bore with pills and symptom check-lists. There is no single form of Psychiatry today and many shrinks my age have never perused the DSM unless to find a plausible insurance code.
Word to the wise: Some shrinks want to understand you in depth, some want to diagnose you and give you pills, and some try to tailor help to you as an individual with talk therapy and/or medicine if needed. Many patients do not wish to open their hearts and souls - it feels too threatening and often is - and just want a pill if it will help them feel better without having to think too hard. My approach is to try to understand a person first but, if they want to try a pill, fine.
Here's something: The Medication Generation - Many young people today have now spent most of their lives on antidepressants. Have the drugs made them 'emotionally illiterate'?
The official Maggie's Farm Weight Loss plan eliminates carbs for the same reason: even minor carbs give you an insulin spike which undoes any conscientious diet effort. If you cannot grow some spine and resist carbs, just give up on your weight issue because it ain't gonna happen.
Parts 1 and 2 were re-posted over the past two days.
I mentioned in an earlier post that a person's ability to adjust reasonably well to adult life does not necessarily depend on their DSM diagnosis (if they have one), but instead on their personality traits. Most of the personality traits we observe in people have to do with what we call "ego functions."
For just a few examples, what is their physical, mental and emotional stamina and endurance? What is their stress-tolerance, and how easily are they overwhelmed? How good are they at assigning themselves tasks and completing them? Are they reasonably honest, or connivers? What are their relationships like, and what sorts of relationships do they like to have? Are they socially appropriate? How sound does their judgement seem to be? How do they do with maintaining boundaries? How smart are they? How flexible is their thinking? How do they do with delaying gratification? Are they reliable or erratic? How self-regulating are they, or do they depend on external structures to function well? How often do they make excuses or blame? What do they want out of life? What motivates them? Do they have wholesome outlets? Are they emotionally mature? How do they view themselves, and how consistent is that with the reality?
Furthermore, what traits are out of line and give the person trouble managing life?
As I mentioned before, it is foolish to hold any standard of human perfection: I call that Psycho-utopianism. Let's just say that we are interested in a person's profile.
For the final post on the topic pf Psychiatric Diagnostics, let's take a closer look at Leo Bellak's list of ego functions, from Dr. Blatner's site which I linked last week. (It's not the best list. I wrote up a better one years ago, but cannot find it.)
1. Reality Testing: This can range from Disorientation to Distortion to Accurate Perception. Lots of seemingly normal people don't really check out their impressions of reality and operate with mild to moderate levels of distortion! 2. Judgment. This can range from "Infantile Omnipotence"--that sense that if I want to do it, I can-- to a more sophisticated Degree of Appraisal of Consequences. Even political leaders can lack this. Again, many of these variables are not always at the top end for many adults. 3. Sense of Reality. Most people sense their objective reality and can differentiate it from dream. 4. Regulation/Control Affects/Impulses: This can go in either the directions of being too impulsive or on the other hand, too over-controlled. With maturity and health, people learn to vary the degrees of control, allowing spontaneity in some settings, being more low-key in others, and making the transitions smoothly, but few adults still do this very well, enjoying full spontaneity; many are all too habitually self-controlled. A few allow themselves to be excessively impulsive regarding anger, or shopping, or in dealing with sexual temptation, etc.. 5. Object Relations: What is the person's capacity to engage in a caring or close relationship, with a romantic partner, a good friend, family members, or close co-workers. Does the person tend to be excessively detached or, again, going to the other extreme, overdependent? Do they shift among these positions, playing a lot of what Eric Berne would call interpersonal "games"? (i.e., what used to be called "neurotic.") Or can they engage with mutuality and flexibility? 6. Thought Processes. This variable includes not just intelligence, but also psychological states that avoid the anxiety of thinking, so they fail to engage in abstract reasoning. Or can they, instead, manage conceptual thinking? Many people are in the middle on this one. 7. Adaptive Regression in Service of Ego (ARISE): This is a fancy psychoanalytic term to explain the capacity to enjoy imaginativeness, the innocence of daydreaming, the freedom of the best of childhood's pretending and playfulness. The lack of this can itself add a good deal of rigidity to the personality. 8. Defensive Functioning: Some people use more mature defenses, humor, sublimation, suppression, and the like. Others tend to use more habitual, automatic, and immature defenses, sometimes even fairly primitive ones that waver on the edge (or go over the edge) of mental illness. 9. Stimulus Barrier: Some folks are hypersensitive, others too dense. To the extent that one is over-sensitive, what coping maneuvers are they capable of to compensate for this sensitivity? 10. Autonomous Functioning. Aside from any emotional issues in life, how competent is the person, or free of pervasive inner conflicts, so that they're able to perform daily tasks regarding personal hygiene, communicating with others, being able to do simple or more complex work roles. Many people are pretty functional, but sometimes blocked if they're upset. Some have developed healthy--and occasionally unhealthy--abilities to resist any intrusion of personal issues on their hobbies or work skills. 11. Synthetic-Integrative Functioning. Some folks are fairly good in one area and terrible in other areas. How well can they manage to integrate all the other variables being spoken about here? 12. Mastery-Competence: Some people have low initiative and are under-achievers. Others may have significant emotional wounds, but yet able to perform remarkably well in work, sports, and so forth. 13. Superego Adaptation. Again, this can be too much, or too little, strongly blaming oneself, or shockingly lacking in guilt or shame, tending toward the puritan or happy-go-lucky type. More mature people are able to acknowledge errors and seek to rectify them, moving toward a more balanced type of social conscience. 14. Strength of Drives: Some people are more sexual than others, and in some cases this may be more extreme in either direction, from the asexual to the hyper-sexual or driven. This can be affected by hormones, overstimulation, and other factors. Another drive is the aggressive, which can be diverted into hostility, grumpiness, or more focused as competition and work. Other people are less driven, and at the extreme, "un-motivated."
When we try to assess these things, we know that we are looking at surface manifestations, not at what is going on in depth. Like geologists gazing at a landscape, we speculate about what is underground based on what we see above ground, and then test our speculations with test drilling.
Modern Psychiatrists and Psychoanalysts often tend to focus on the "Object Relations" item, believing that, developmentally, the integration of mental relationships effects the stability and integration of the adult person (and that aberrations can be improved with Psychotherapy). I am a friendly skeptic about that, and more inclined towards the genetic basis of personality traits (which by no means implies that they are immutable).
OK, I am going to avoid depth psychology here because my purpose with these posts was to give a sense of the sorts of things shrinks think about when they evaluate somebody and not about Psychotherapy or Psychoanalysis. As for the medical students who will not specialize in Psychiatry, these sorts of methodical ways of thinking about people are quite practical, not especially theoretical, and, I believe, useful to everybody in their dealings with others.
Photo is Anna Freud, the more-or-less founder of Ego Psychology.
(This series is a peek - a few samples - into what goes on in Third-year Psychiatry in Medical School. Very few of the students will select Psychiatry as a specialty, but all do clinical rotations through Surgery, Pediatrics, Internal Medicine, Psychiatry, OB-GYN, etc. - and further elective rotations in the 4th Year. I focused on Surgery and Orthopedic Surgery in my 4th Year. The Surgeons did their best to win me over, and almost did.)
In one of the teaching sessions, we watch a video of a half-hour intake interview of a patient in the Internal Medicine clinic, done by a third-year medical student. At the end of it, I ask "Let's list everything we now know, or might speculate about knowing, about this patient."
We go through the medical history, the patient's demeanor (what's their style? Dramatic? Passive? Grouchy? Warm? Arrogant? Sneaky? etc), physical appearance, dress, posture, eye-contact, tone of voice, nature of his interaction with the interviewer, apparent intelligence, knowledge about health issues, work history, family, special concerns, and so forth.
The students who have been science nurds and wizards are often astonished by how much information can be collected from a simple half-hour medical - non-psychiatric interview. I write it all down on the whiteboard, some as facts and some with a ?.
It usually fills the entire board, especially if I write large enough.
In Psychiatry, we have no high tech diagnostic tools - just our eyes and ears.
Moving to Psychiatry, let's assume that we are meeting with a patient in the Psychiatric consulting room - a new patient who does not require any sort of acute crisis intervention or triage. What do we want to know about this new patient right away, after they tell us why they are here?
First things first. We want to know about their general health. That is from their story, and via eyeball. (Over the years, I have diagnosed hypothyroidism, brain tumors, Lyme disease, MS, GI cancers, Parkinson's Disease, early Dementia, etc. in people who have come to me for Psychiatric help).
Then the obvious things. Their life story, their family history, their current life situation. We assume we are never getting the whole story, but we need a provisional frame for the picture. In the process of asking our questions and following up topics of interest, there are a number of other things we get from initial interviews, using our bag of tricks and our sensitive ears, which are solid data.
For some examples:
- We determine how self-observing they are, their capacity for "insight" - We determine their motivation to deal with their problem - We usually get a provisional DSM Axis 1 diagnosis - if they have one - We get an idea of what their coping devices are, and when and how they fail - We get a good idea of their IQ, their life skills, fund of knowledge, their adaptive success - what we call their "ego strengths" and level of functioning in important areas of life (eg relationships, work, avocations, etc) - We get a sense of how they relate to others (to us, being the case at hand), rapport, relatedness, and a sense of what their personality is like, their appropriateness, manners, boundaries, attentiveness, sense of humor, etc. etc. - We would like to be able to say something about the style of their thinking, and especially their patterns of defenses - We would like to know how they respond to our observations and comments (eg defensive? interested? insulted? embarassed?) - Try to assess their morality and impulse control, reliability, and any sociopathy or secondary gain, or manipulativeness (this can be difficult but, with experience, one can smell it)
(These are the sorts of observations that make some folks uncomfortable with shrinks in social settings. People are often not aware that when we shrinks are out of the office, we probably think about these things less than the average person. For us, it's work.)
The point is that the Psychiatric interview is just a variant of the medical interview, but one which usually takes more than a half hour. Sometimes, much more. With healthy patients with neurotic problems, sometimes it can take me 5 or 6 one-hour meetings just to come up with a provisional case formulation and treatment plan (if needed). With very ill patients, 3 minutes can be enough to make a triage plan (eg Agitated guy fighting with security guards and cops yelling that they are CIA trying to implant more transmitters in his brain. Easy. Get the guards to hold him down and give him IM Haldol and Ativan with a little Cogentin...and wait a while.)
What's our goal? Our goal is a thorough Psychiatric Diagnosis and a Case Formulation. In medical school, in Psychiatric Residency, and in an Analytic Institute you have to write these up as lengthy formal presentations, but at my stage you just kinda do it in your head and store it in your head, except in special circumstances.
As rank amateurs, medical students cannot be expected to do either of these in an expert way, but we require that they produce a couple of these on some of the patients they are following.
These posts are bits from a short series of presentations which I give to medical students during their required Third Year Psychiatry rotations. Which is to say, it is more or less directed to the general public but oriented towards general-physicians-to-be.
(Very few of these medical students will choose Psychiatry as a career, given all of their choices. More of them will chose Radiology than Psychiatry - wherein they will have plenty of fun and much to learn but never even have to talk to a patient at all - or Dermatology, wherein they will never have to be on call for the hospital. However, most will select Internal Medicine for their internships, which itself is a path to other specialties. FYI, all American-trained Psychiatrists do internships which include Internal Medicine or Pediatrics, plus Neurology, and get Board certification from the American Board of Psychiatry and Neurology.)
My presentation is not about making specific diagnoses (that comes from other Profs) - it's about the preliminaries: how all Docs can think about their patients, if they want to, and how shrinks think about their patients.
It's partly meant to be a corrective to the often-stated idea that the DSM is any gold standard of diagnosis, and it is meant to encourage young docs to think about their patients' lives, not just about their diagnoses - whether psychiatric or otherwise. And if I can interest them in the sorts of things shrinks think about, and gain some appreciation for what shrinks do, so much the better.
My presentation is based on the idea that, in the end, the job we shrinks get paid to do is to figure out what interferes with a person's ability to make a reasonably mature and effective adjustment to life if they wish to do so, and to try to reduce pathological mental pain, impairment, and anguish (but not healthy pain, worry, and anguish, like guilt, regret, sadness, realistic anxiety, or grief).
It's not to try to make people "normal," because "normal" doesn't really apply. People are wonderfully different, each with his own unique fingerprint of strengths, weaknesses, neuroses, interests, abilities, ego strength profile (about which more later), etc. In fact, unusual characters are a fine addition to the fabric of life.
I usually end my first session with a case example, for example, of a 42 year-old patient with hypertension coming in for a routine follow-up with his internist or GP. He has been prescribed 20 mg of Coreg/day for a month, and his systolic BP is 170 (had been 180 at his last visit).
I do my rapid-fire Socratic shtick. I ask them "So, Doctor, what do you want to know about this guy?"
"Is he compliant with the meds?" somebody wonders.
"Compliant!" I say. "What is he, your servant?" "Isn't the right question whether he is concerned enough about it to take the pills every day? Whether he can afford the meds? Does he need your free samples? Whether his life is too disorganized to do it? Whether it's the right medicine or the right dose? Or whether he even cares?"
We go on like this for around ten or fifteen minutes, and end up constructing a picture of a middle-management sales guy who is recently unemployed, divorced with two kids, mildly depressed, worried about money and alimony and child support, living in a small rented condo with rental furniture on take-out junk food and Chinese food, with some tendency for denial because he feels overwhelmed, with some deterioration in his self-care since his divorce made worse by the lack of structure and discipline in his unemployed life. His BP is the least of his concerns, but he does want to maintain a good relationship with the Doc, who he views as a friend and as a caring emotional support.
You rapidly move past the notion of A Case of Hypertension to the uniquely human and individual. It's good fun for all of us, and a good break for them from the fascinating but mechanistic details of caring for the renal functions of unconscious gomers in the ICU. It's about the art of doctoring, not medical science. You cannot do medicine "by the book," because each patient is his own book.
Then I tell them that they have just made a first step towards Real Psychiatric Diagnosis - and the real practice of clinical, office medicine as opposed to our equally wonderful technological medicine. It's about wondering "Who is this person who is asking me for help?" and not just about "What ails them?" After all, hypertension is painless, and doesn't really "ail him" at all. If you want to help this guy, all of this information about him might be useful to you.
In conclusion, I warn them that the same thing applies to Psychiatric diagnostics. Some people with Schizophrenia - a dread and incurable disease - have more satisfactory lives than some addicts - a sort-of fully curable problem. People are complicated, and so, often, are their lives.
Then I command the students to read MacKinnon and Michels' The Psychiatric Interview as their first of several readings for my series. A Psychiatric interview isn't much different from any other medical consultation with a new Internist or Family Doc, really - except no physical exam other than that of the well-informed medical eyeball (which can detect a lot).
Yes, I will interrogate them on their readings just as the Surgical Profs do with their text on the examination of the abdomen, or Neurologist Profs do with the diagnosis of stupor and coma (or, as we termed it in medical school, the Diagnosis of Stupor, Coma, and Death. Funnily enough, the diagnosis of death isn't always so easy).
Parts 2 and 3, and maybe 4, later. Why am I posting this? To help me collect my thoughts and to improve my presentations.
Photo is Dr. Emil Kraepelin, father of modern Psychiatric diagnosis who, among many other things, distinguished Manic-Depression from Dementia Praecox (Schizophrenia).
For every person who says “I’m unhappy” there must now be a thousand who say “I’m depressed.” The change in semantics is important: the person who says he is unhappy knows that there is something wrong with his life that he should try to alter if he can; whereas the person who says “I’m depressed” is ill, and it is therefore the responsibility of someone else — the doctor — to make him better.
For the sorts of Psychiatrists who find it valuable to probe below the surface, there are many sorts of depression and many causes. Even grief can sometimes lead to a debilitating depression.
In my private office, the most common "cause" of agonizing, if not always debilitating, depression is narcissistic injury. These patients often can benefit enormously by psychotherapy alone, and can end up far healthier and stronger than before.
It's difficult to study something that nobody can define in a non-circular way. From McCloskey: Happyism - The creepy new economics of pleasure. She makes the point that much of this is pseudo-scientific.
A quote from her very interesting essay:
...in the eighteenth century, our earthly happiness became important to us, in high intellectual fashion. By 1776, “life, liberty, and the pursuit of happiness” was an unoriginal formulation of what we all, of course, now admitted that we chiefly wanted. John Locke had taught, in 1677, that “the business of men [is] to be happy in this world by the enjoyment of the things of nature subservient to life, health, ease, and pleasure”—though he added piously, “and by the comfortable [that is, comforting] hopes of another life when this is ended.” By 1738, the Comte de Mirabeau wrote to a friend, recommending simply, “[W]hat should be our only goal: happiness.”
“Our only goal.” To see how strange such a remark is, consider whether it could have been uttered by a leader of opinion in 1538. Martin Luther? Michelangelo? Charles V? No. They sought heavenly, artistic, or political glory—not something so domestic as happiness. Yet, in the late seventeenth century, even Anglican priests commenced preaching that God wanted us to be happy as much as holy. They called it “eudaemonism.” Anglicans and, astonishingly, some New England Congregationalists turned against the old, harsh, Augustinian-Calvinist line. We are not, declared the eudaemonists, mere sinners in the hands of an angry God, worms unworthy of grace. We are God’s beloved creatures, his pets.
The eudaemonistic turn was a Very Good Thing, resulting in fresh projects to better our stay here on Earth, some of them remarkably successful. Democracy was one, since, if you followed the fashion for universal happiness, it became impossible to go on insisting that what really mattered was the pleasure of the Duke or the Lord Bishop. Enlightened despots of the era claimed to seek the good of all, which paradoxically gave the populace the idea that maybe they themselves could do it.
I will remind our readers that Freud (yes, still relevant in many ways but not in all ways) had a somewhat tragic view of life and figured that pleasure and joy certainly matter, but that, overall, ordinary - "non-neurotic" - unhappiness is man's fate. Some days, I agree with that, other days, I don't.
By coincidence, Schneiderman's Unhappy or Depressed? I will need to return to the Dalrymple piece he quotes, later.
Probably for confidentiality reasons, Dr X took a fictional character as a sample rather than trying to camouflage a real patient. This is my idea of a real diagnostic impression of a patient without a major illness (eg dementia, schizophrenia, narcotic addiction, melancholia and major depression, bipolar disorder, etc.).
He briefly covers the defensive structure, the character structure, the basic conflicts as they relate to the person's life. Outside the major ailments, the DSM is useless in depicting a patient - a person with his flaws and weaknesses. In these times of the the low-rent superficial, check-list, cook-book Psychiatry, I find internists often more interested in the whole person than some Psychiatrists who just want to give you the right pill without delving into your psyche beyond the surface complaint. In my view, that is not serious medical practice. I do not approve of it, nor do I think it is cost-effective in the end. Some people are attempting to hyper-medicalize and simplify my field of work, but the human soul is too complex for that to work most of the time.
My field is deeply divided these days. It makes things interesting, controversial, and sort-of fun.
Unlike Dr. X, I never write these things down anymore. It takes too much time, can be subpoenaed and distorted in divorce court (some bad experiences with that before I quit writing things down), and otherwise nobody will ever read it before it is shredded. However, I store them in my brain. My brain has plenty of storage capacity.
I will re-post, for those who might be interested, my series on serious diagnosis over the next few days.
Character is destiny. Mostly, except for bad luck.


 Deirdre McCloskey on
Deirdre McCloskey on 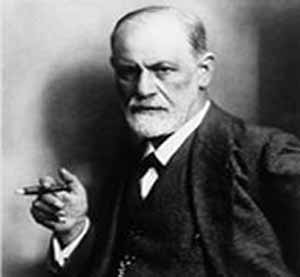 "The narcissism of small differences" was Freud's
"The narcissism of small differences" was Freud's 
 I happen to believe, based on experience, that the right psychotherapeutic approach, tailored for the individual, can be enormously helpful.
I happen to believe, based on experience, that the right psychotherapeutic approach, tailored for the individual, can be enormously helpful. 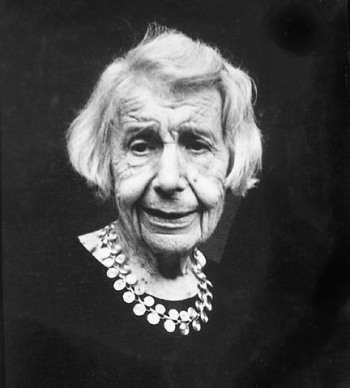 Parts 1 and 2 were re-posted over the past two days.
Parts 1 and 2 were re-posted over the past two days. Part 1 was re-posted yesterday
Part 1 was re-posted yesterday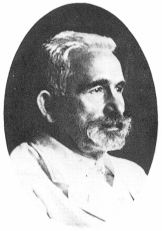 These posts are bits from a short series of presentations which I give to medical students during their required Third Year Psychiatry rotations. Which is to say, it is more or less directed to the general public but oriented towards general-physicians-to-be.
These posts are bits from a short series of presentations which I give to medical students during their required Third Year Psychiatry rotations. Which is to say, it is more or less directed to the general public but oriented towards general-physicians-to-be.