There are four data that the public is interested in for epidemics: Exposure %, mild illness %, truly ill %, and dead %. But % of what? Journalists have no clue about this.
Exposure can be tested, whether ill or not. However, very few people will be tested for exposure if they feel fine or have the sniffles, and it would be absurd (except for a limited study of the general population) to randomly test people. I'd be interested in those results but it's academic.
One epidemiologist said yesterday that the majority of people in the NYC metro area (NY, NJ, CT) and in MA have been exposed. A guess, though. Exposed but not ill is good. You get herd immunity. It is happening now, for sure. Probably in CA too. Most viral spread is probably by people without symptoms who assume they are clear.
My point is that, without a number for people exposed and unexposed within a given general population, you have no denominators. If the only data you have is dead people (not many thus far) divided by sick people getting tested, you have minimally-useful information from a public health standpoint. From a doctor's standpoint, it's useful to know risk of sick to dead even though there is no treatment, other than supportive, for viral pneumonia.
So what is a "death rate" based on in the absence of relevant data, ie deaths/exposed? So the danger of this virus, right now, can not be determined or even estimated. That might be knowable in a few months.
I am not an ID doc, so I'll just tell you what I am doing. I am hoarding nothing. I am taking walks or hikes daily in the sunshine. I wash my hands, but I always did. I am going to the gym and working out (improves immune response). I am not going to church (because it's closed at the moment.) Small meals are my normal anyway (improves immune response and generally healthier).
If you've been exposed (probably) and feel entirely well, you are still infectious but if you aren't coughing or sneezing, it's sort-of ok.
We'll all be fine, unless frail, with preexisting serious ailments, or elderly. Those things apply also to the ordinary seasonal flu. However, there is really no way to insulate them because staff help, family help, etc. can be exposed but without any symptoms. There have been a few cases of otherwise healthy people becoming ill enough to need hospital care, but not many.
Please correct my thinking if I am in error.
This makes sense to me: Coronavirus going to hit its peak and start falling sooner than you think.
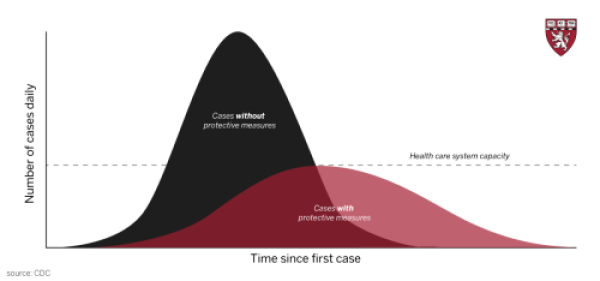
As we have said before, the goal is to try to flatten the exposure curve (speed of exposure), not to prevent exposure because that really cannot be done unless you isolate on an island somewhere for 6 months.
Addendum: Flattening the curve of an infection slows the rate of exposure. But how is a "case" defined?